3 Draining Veins The most basic and important tenet of arteriovenous malformation (AVM) surgery is that the draining vein must be preserved until the very end of the resection. It seems counterintuitive in the presence of ferocious arterial afferents to place efferent veins at the center of the AVM dissection strategy. It also seems contrary to aneurysm surgery, which places afferent arteries at the center of the dissection strategy. Aneurysms originate from the afferent artery and are controlled by proximal temporary occlusion. When an aneurysm ruptures intraoperatively, the catastrophe is managed by tamponading the dome, suctioning the field, and occluding afferent and efferent arteries with temporary clips. Gaining arterial control enables permanent clipping of the aneurysm. In contrast, AVMs rupture intraoperatively when venous outflow is occluded prematurely by mistake. Intranidal pressure increases, the AVM distends, and before long it ruptures and torrential bleeding floods the surgical field. There is no orderly sequence of winning maneuvers as there is with aneurysm rupture. Tamponade is ineffective because there are multiple bleeding sites, suction may not clear the field, and afferent arteries are too numerous to control quickly or completely. Therefore, absolute preservation of the efferent vein must always be the first priority in AVM surgery. Arterial afferents may be the source of nasty bleeding during the resection, but they are not the cause of AVM rupture. Although they must all be isolated, occluded, and divided eventually, they are not at the center of AVM dissection strategy. The secret to preserving draining veins is not mistaking them for feeding arteries. Color is usually the most striking difference between artery and vein, but AVM draining veins and feeding arteries are both bright red. Therefore, color is deceptive and cannot be trusted. Size is a more reliable distinguishing feature. Although some veins or varices are massively dilated with no question about their true identity, others are merely large and resemble a dilated artery. However, arteries dilate only so much, even when feeding a high-flow AVM with fast intranidal shunts. Thick smooth muscle cell layers and elastic laminae limit the distension of feeding arteries, such that they rarely exceed diameters of 4 mm. Veins, on the other hand, are little more than an endothelial lining of intima, a thin layer of smooth muscle cells in the tunica media, and some collagen fibers in adventitia. Veins situated on the receiving end of an arteriovenous shunt enlarge easily. Therefore, any vessel greater than 4 mm in diameter, no matter how cylindrical or “arterial” it appears, is a vein until proven otherwise. These structural differences between arteries and veins can be detected under the illumination and magnification of the operating microscope. The muscular striations in thicker arterial wall can be visualized directly, and they mute the color of arteries to slightly pink. The lack of smooth muscle cells in thinner venous wall imparts a smooth uniformity and a brighter red color. Additionally, thin venous walls are more translucent, and the mixing of oxygenated and deoxygenated blood can be observed through them. Such mixing does not occur in arteries and cannot be observed through their thicker walls. Following a vessel as it leaves an AVM may help determine its identity. Arteries dive into sulci and fissures as they are traced proximally, whereas veins rise to cortical surfaces en route to sinuses. An arterialized vein merges with normal venous tributaries, with mixing of darker blood at their confluence. In contrast, an artery bifurcates and sends pial branches to adjacent cortex, and there is no such mixing. Temporary “test” occlusion of a vessel with a forceps or temporary clip will darken a vein distal to the occlusion but not an artery. Embolic agents like glue, Onyx, polyvinyl alcohol particles, and coils are easy clues to a vessel’s arterial nature, but they create a paradoxical color reversal that darkens feeding arteries with intraluminal thrombus while an adjacent vein remains bright red. Aggressive embolization with newer agents like Onyx may nearly occlude the AVM, to the point that even an active draining vein may be almost normal in color. The urge to attack an AVM and subdue a big feeding artery is strong. However, that urge must be countered by scrutiny of the vessel and all its morphological nuances. Before committing to occlusion, ask, “Is it artery or is it vein?” In addition, know the veins that are in play for each AVM subtype (Table 3.1). Table 3.1 Summary of Veins in the Seven AVM Locations
 Absolute Preservation
Absolute Preservation
 Recognizing Veins
Recognizing Veins
Abbreviation | Vein |
Frontal veins |
|
FrPolV | Frontopolar vein |
AntFrV | Anterior frontal vein |
MidFrV | Middle frontal vein |
PosFrV | Posterior frontal vein |
PreCenV | Precentral vein |
CenV | Central vein |
MedFrV | Medial frontal veins (anterior, central, posterior) |
PcaV | Pericallosal veins (anterior, posterior) |
FrSylV | Frontosylvian vein |
SupSylV | Superficial sylvian vein |
DeepSylV | Deep sylvian vein |
OrbFrV | Orbitofrontal vein (anterior, posterior) |
OlfV | Olfactory vein |
Temporal veins |
|
AntTempV | Anterior temporal vein |
MidTempV | Middle temporal vein |
PosTempV | Posterior temporal vein |
Labbe | Vein of Labbé |
TempBasV | Temporal basal vein (anterior, middle, posterior) |
UncV | Uncal vein |
HippoV | Anterior hippocampal vein |
MedTempV | Medial temporal vein |
BVR | Basal vein of Rosenthal |
Parieto-occipital veins |
|
PosCenV | Postcentral vein |
AntParV | Anterior parietal vein |
PostParV | Posterior parietal vein |
OccV | Occipital vein |
Trolard | Vein of Trolard |
ParaCenV | Paracentral vein |
MedParV | Medial parietal veins (anterior, posterior) |
AntCalcV | Anterior calcarine vein (internal occipital vein) |
PosCalcV | Posterior calcarine vein |
PcaV | Pericallosal veins (anterior, posterior) |
SplenV | Splenial vein |
OccBasV | Occipital basal vein |
Ventricular and deep veins |
|
SepV | Septal vein (anterior, posterior) |
CauV | Caudate vein (anterior, posterior) |
ThaStrV | Thalamostriate vein |
ICV | Internal cerebral vein |
AtrV | Atrial vein (medial, lateral) |
ChorV | Choroidal vein (superior, inferior) |
VoG | Vein of Galen |
Brainstem veins |
|
MAPonMesV | Median anterior pontomesencephalic vein |
MAMedV | Median anterior medullary vein |
LAPonMesV | Lateral anterior pontomesencephalic vein |
LAMedV | Lateral anterior medullary vein |
LMesV | Lateral mesencephalic vein |
LMedV | Lateral medullary vein |
ReOlvV | Retro-olivary veins |
PedV | Peduncular vein |
PComV | Posterior communicating vein |
VPonMesS | Vein of the pontomesencephalic sulcus |
VPonMedS | Vein of the pontomedullary sulcus |
TrPonV | Transverse pontine vein |
TrMedV | Transverse medullary vein |
MPMedV | Median posterior medullary vein |
TecV | Tectal vein |
Cerebellar veins |
|
IHemV | Inferior hemispheric vein |
SHemV | Superior hemispheric vein (anterior, posterior) |
AHemV | Anterior hemispheric vein |
SVerV | Superior vermian vein |
IVerV | Inferior vermian vein |
PreCenCblV | Precentral cerebellar vein |
TonsV | Tonsillar vein |
ReTonsV | Retrotonsillar vein |
SPetrV | Superior petrosal vein |
IPetrV | Inferior petrosal vein |
VCPonF | Vein of cerebellopontine fissure |
VCMedF | Vein of cerebellomedullary fissure |
VCMesF | Vein of cerebellomesencephalic fissure |
Sinuses |
|
CavS | Cavernous sinus |
SphParS | Sphenoparietal sinus |
SSS | Superior sagittal sinus |
ISS | Inferior sagittal sinus |
SPS | Superior petrosal sinus |
IPS | Inferior petrosal sinus |
StrS | Straight sinus |
SigmS | Sigmoid sinus |
TrvS | Transverse sinus |
SphBasS | Sphenobasal sinus |
SphPetS | Sphenopetrosal sinus |
Torc | Torcular |
TentS | Tentorial sinus |
 Compass and Odometer
Compass and Odometer
Approximately one third of AVMs are beneath the cortical surface and two thirds have superficial venous drainage, which means that many of these subcortical AVMs have only an arterialized vein on the surface. The vein, therefore, becomes a compass that guides the dissection to the nidus. Dissecting along a draining vein from the outset is inherently risky; one wrong move can injure it, induce bleeding before even seeing the AVM, or compromise outflow in the process of controlling the bleeding. Distended veins are difficult to get around because of their large size, requiring gentle traction with a sucker or mobilization back and forth (dynamic retraction). As the dissection deepens, the vein can obstruct the surgical field. For example, some sylvian AVMs are covered by superficial sylvian veins and must be dissected between branches in this complex. Similarly, medial frontal and medial parieto-occipital AVMs are covered by medial veins that ascend and bridge to the superior sagittal sinus, which not only crowds the surgical corridor but also may tether the hemisphere and neutralize the benefits of gravity retraction. When superficial veins become obstacles, they are easily injured by passing instruments or fixed retractors. When attention is focused deep in the field, it is easy to lose sight of these veins. Veins are preserved by shifting the dissection to either side, connecting planes beneath the veins, keeping them irrigated and unstretched, and maintaining peripheral vision with less magnification on the microscope.
The draining vein also becomes an “odometer” that measures the progress of the resection as its color changes from red to purple to blue. The vein offers a visual signal throughout the case. Dramatic color changes do not occur until the later stages of resection, but quieting of AVM hemodynamics can sometimes be appreciated in the earlier stages through the window of the odometer. A stubbornly red vein is a clear signal that important arterial input remains. Persistent arterialization of the vein may result from incomplete circumdissection of a deep plane, deep perforating artery supply, or feeders hiding along the underbelly of the draining vein. Even small contributions from deep perforating arteries keep the draining vein of a large AVM surprisingly red. Red veins mean that the fight is still on, and blue veins are the AVM’s white flag of surrender.
 Secondary Veins
Secondary Veins
The tenet of absolute preservation of the draining vein applies to the primary vein, the main one that collects most of the AVM’s outflow (Fig. 3.1). Each AVM subtype has a predictable primary vein that can be anticipated (Table 3.2). In addition, many AVMs and especially the large ones have multiple draining veins radiating in different directions. Arteriovenous malformation outflow distributes within the nidus and communicates with these draining veins, and preservation of every draining vein until the very end of AVM resection is not necessary. In other words, a secondary draining vein can be sacrificed safely during the resection without precipitating AVM rupture. This requires first designating the primary vein to be preserved, and second sufficiently reducing arterial input with a combination of embolization, feeding artery occlusion, and circumdissection.
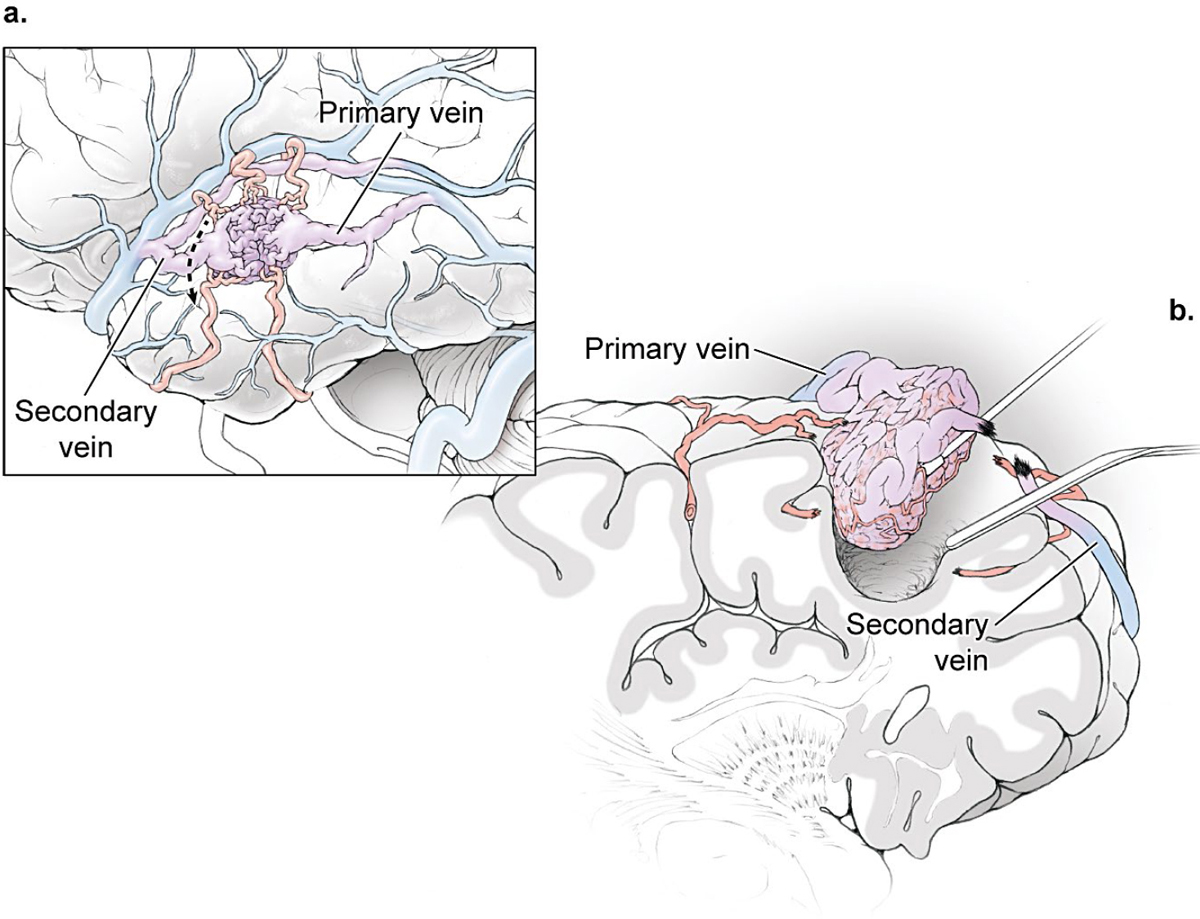
Fig. 3.1 Preservation of the draining vein is the most important tenet of AVM surgery. (a) The AVMs with multiple draining veins require designating a primary draining vein that must be preserved and secondary veins that may be sacrificed during the resection as arterial input is reduced. (b) Venous trimming de-tethers the AVM and advances circumdissection.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


