Both studies that investigated the use of self-modelling in conjunction with speech restructuring (Cream et al., 2009, 2010) reported positive changes in self-reported severity ratings. Taken together, they therefore provide support for the notion that self-modelling may contribute to the generalisation of treatment effects; particularly considering that one of them warrants interpretation as a clinical trial. Overall satisfaction with fluency and reduced impact of stuttering may be related to a change in perceived self-efficacy.
A limitation of all the evidence presented here is that self-efficacy is theoretically considered to be underpinning self-modelling treatment, however, none of the studies reviewed have measured it. In summary, although the objective measures do not give a consistently positive result, the self-report measures demonstrate some value of self-modelling for chronic stuttering. The evidence from these six studies shows that there is great potential for self-modelling as an adjunct to speech restructuring treatment for chronic stuttering.
Advantages and disadvantages
Advantages
Self-modelling for chronic stuttering is a simple and cost efficient treatment that has potential to reduce stuttered speech, particularly following speech restructuring treatment. Self-report measures indicate it has potential to promote both generalisation and maintenance of speech outcomes. It appears that all clinicians need to do to potentially bring these benefits to clients is to supplement their treatments with a self-modelling video recording. There are striking cost efficiencies to such a procedure. Arguably the literature reviewed suggests that self-modelling may be particularly applicable to the problem of post-treatment relapse. If the findings of Cream et al. (2009) can be replicated, it is conceivable that all clients could finish their treatments armed with a self-modelling video, and it could be used to restore stuttering control as needed. Perhaps the problem of post-treatment relapse may be considerably diminished if clients were to regularly review their self-modelling recording.
Disadvantages
The disadvantage of self-modelling is that clients need to have the ability to produce reasonable amounts of stutter-free speech for their self-modelling recording. Beyond that practicality, based on the evidence presented here, self-modelling appears to be efficacious for stuttering clients who have already learned a speech restructuring technique to control stuttered speech. At least judging from the Webber et al. (2004) results, those who have never learned any technique for stuttering control do not respond as favourably as those who have received some such treatment. It is also the case that the clinical trials reported here show a modest effect size. If further clinical trials affirm that indeed such an effect size is all that is realistically attainable with self-modelling, then, considering that such effects can be attained without any clinical cost, then they would be worth having nonetheless.
Conclusions and future directions
There is considerable potential for self-modelling as an adjunct treatment for stuttering. Nonetheless, there are many targets for further investigation. There are three research directions from now that would guide clinical practice. The first relates to the theory that underpins self-modelling. Can the self-efficacy changes that relate to self-modelling be measured? At present it is assumed, rather than proven, that the benefits of the procedure during stuttering treatment are related to such changes in self-efficacy. If it can be shown that this is the case, then clinicians could focus more specifically on self-efficacy during self-modelling as an adjunct treatment to stuttering. Second, and most fundamentally, further clinical trials research is needed to verify the potential benefits of the procedure. Using a liberal definition of a clinical trial, only one has been reported. Independent replication of clinical trials results is essential to bolster clinician confidence in that result. Finally, it seems to be a general rule of stuttering treatment that interventions are more efficacious for younger participants, but that does not appear to be the case with self-modelling. That certainly requires continued research.
It has been demonstrated that even a brief delay between performance and observation reduces the instructive value of the self-modelling (Carroll & Bandura, 1985; Fireman, 1996). Performance is enhanced, however, when video feedback is provided simultaneously with a behaviour that could otherwise not be observed by the person (Carroll & Bandura, 1982). For example, simultaneous self-modelling displays presented in a mirror rather than by video have been used in conjunction with negative practice to reduce the frequency of facial tics (Frederick, 1971). An early recommendation by Van Riper (1973) was that those who stutter should read in front of a mirror. Subsequent investigations of this idea (Hudock et al., 2011; Snyder et al., 2009) suggested some merit in it, and a programme of research at the Australian Stuttering Research Centre has begun to explore it further.
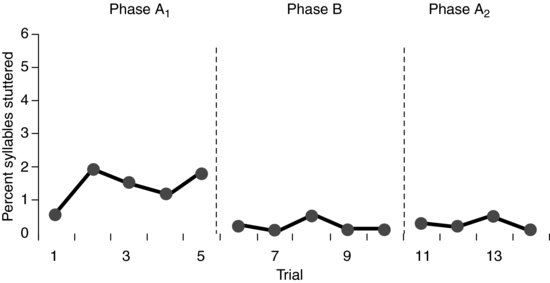
Our progress to date is an experiment with ten stuttering clients, five of whom had previously learnt a speech restructuring technique to control stuttering and five of whom had had no previous treatment. A time series single subject ABA design was used. The A1 phase involved speaking in monologue for 3-minute trials, the B phase involved speaking in monologue for 3-minute trials while looking into a mirror and the A2 phase was a repeat A1 phase. Eight participants completed the experiment and for seven of these, no effect on stuttering from mirror self-modelling was evident. However, stuttering did reduce for one participant who had previously learnt a speech restructuring technique to control stuttering. Results for this participant are presented in Figure 12.2. We are not sure yet what to make of this modest finding, but there is some possibility that further research will show that for some clients who experience post-treatment relapse, mirror self-modelling may be a useful technique.
Figure 12.2 Results for one of the successful participants from our preliminary investigation of mirror self-modelling.
Related posts:
 Assessment and Treatment of Stuttering Using Altered Auditory Feedback
Review of the Successful Stuttering Management Program
Multifactorial Treatment for Preschool Children
Assessment and Treatment of Stuttering Using Altered Auditory Feedback
Review of the Successful Stuttering Management Program
Multifactorial Treatment for Preschool Children
 Intensive Speech Restructuring Treatment for School-Age Children
The Gradual Increase in Length and Complexity of Utterance Program
Innovations, Watersheds and Gold Standards: Concluding Symposium Reflections
Intensive Speech Restructuring Treatment for School-Age Children
The Gradual Increase in Length and Complexity of Utterance Program
Innovations, Watersheds and Gold Standards: Concluding Symposium Reflections
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


