Use and abuse of alcohol and narcotics have occurred throughout history. Indeed, until recently their use to alleviate pain was one of the few effective medical therapies. Advances in chemistry led, particularly during the 19th and 20th centuries, to the formulation of more potent preparations as active ingredients were identified and then used to search for other agents. At one time, cocaine and the opiates were widely prescribed and readily available, often being included in various elixirs and tonics. By 1924, an awareness of the potential for abuse led to federal regulation so that opiates and cocaine could only be prescribed by physicians. Similarly, the advent of Prohibition meant that alcohol was no longer freely available; as a result (until repeal in 1933), there was an extensive black market in alcohol as there now is other substances (see Musto, 1999, for an historical review). Over time, the federal government has taken an increasingly active role in the regulation of medications and substances with abuse potential. State governments do, however, continue to be the primary regulators in some areas, e.g., for alcohol sales.
Advances in understanding the pharmacology and mechanisms of action (e.g. using animal models) have advanced our knowledge of brain processes and the mechanisms that may underlie substance abuse. Until recently, most of the work on substance abuse and substance dependence has come from work with adults. There has been less research on children and adolescents. Clearly, adolescents who abuse drugs or alcohol have sure risk for developing dependence in adulthood. Among adolescents, substance abuse is significantly more common than dependence (probably by about two to one), and abuse of multiple substances is fairly common. There is some suggestion (Hopfer & Riggs, 2007) that in contrast to adults, the distinction currently made between abuse and dependency may be more artificial in adolescents.
DEFINITIONS
The Diagnostic and Statistical Manual of Mental Disorder (DSM-IV-TR) (2004) provides diagnostic codes for a host of substance related disorders. Substances of potential abuse include alcohol, amphetamines, caffeine, cannabis, cocaine, hallucinogens, inhalants, nicotine, opioids, phencyclidine, and sedative-hypnotic categories. Other codes provide for polysubstance or unknown substance use/abuse. As a practical matter, in children and adolescents, substance abuse and substance dependence are more frequently encountered (e.g., rather than withdrawal syndromes).
Substance abuse is usually considered a less severe syndrome than substance dependence (the diagnosis of the former is not met if the latter is present). Whereas substance abuse entails impairment of clinical significance caused by use of a substance, dependence involves a number of symptoms reflecting persistent use even in the face of negative consequences. For example, substance abuse involves recurrent use associated with some degree of interference or use in situations in which some danger is involved but without tolerance, withdrawal, and major life impact present. Substance abuse does not entail the same degree of preoccupation with the substance (e.g., worrying where one’s next drink will come from) nor are physiological related to withdrawal present. If the individual meets criteria for tolerance or withdrawal in regard to the substance being abused, physiological dependence is noted as a qualifier.
The various substances of abuse share some similarities as well as many differences in terms of their physiological effects and potential for addiction. Individual factors as well as route of administration all can be important. For some substances (e.g., cocaine), rapid development of dependency may occur. Alcohol is often the first substance adolescents use and accounts for much of adolescent substance use and abuse. In one large national survey, 6% of adolescents met criteria for alcohol abuse or dependence in the previous year. Acute alcohol intoxication is characterized by sedation, slurred speech, decreased heart rate, poor coordination, and reduced blood pressure. Repeated drinking can lead to tolerance and, occasionally, adolescents can even experience alcohol withdrawal states. As with adults, alcohol withdrawal may require emergency medical management. Severe alcohol intoxication can also be an emergent medical problem (e.g., group drinking at parties) and can lead to death at high levels. Impaired judgment and coordination also contribute to accidental death and injuries.
Nicotine in tobacco products can produce dependence and is associated with a number of medical problems. One of the major concerns about tobacco use is its potential for serving as an entry to use of other substances. The effects of nicotine are prompt after inhalation or ingestion (e.g., from chewing) and include central nervous system (CNS) stimulation followed by symptoms of withdrawal. The mechanism of nicotine on acetylcholine receptors is well known. With a half-life of several hours, nicotine can accumulate in the body over the course of the day. Cessation of use can result in irritability, characteristic craving, and problems in mood and concentration.
The most frequently used illicit drug in adolescents is marijuana, and dependence is most frequently cited as the reason for adolescent admissions to substance abuse treatment. About 4% of adolescents meet criteria for use or dependence within the past year. The mechanisms of action of the active ingredients δ-9 tetrahydrocannabinol (THC), has been increasingly studied. This agent binds to the CNR1 receptor which is widely distributed in the brain. Effects on anxiety, appetite, pain are reported as are analgesic effects and enhancement of appetite. Hallucinogenic effects can also be noted. Although the DSM-IV-TR does not recognize a withdrawal syndrome, there is some suggestion that one, in fact, does exist. There is also some suggestion that repeated use may increase the risk for psychosis and other psychiatric problems.
Abuse of heroin and prescription opiates has increased over the past decade and has become the source of increasing concern. One survey suggests that as many as one in 20 high school 12th graders had reported using OxyContin illicitly. The use of various routes of administration of purer heroin, including smoking and snorting, have probably contributed to this increase. Heroin has very significant potential for addiction, and its use is associated with a range of problems impacting adolescents at home and in school.
Cocaine has various psychological effects, including a sense of mental clarity and lack of fatigue. Physical effects include increased heart rate, temperature, and blood pressure as well as dilated pupils. The route of administration leads to major differences in duration of its effects (e.g. smoking leads to a more intense but shorter high than snorting). About 6% of users become dependent within 1 year (Hopfer & Riggs, 2007).
Amphetamines have a long history of legitimate use in medicine, including in the treatment of attention-deficit disorders. About 2% of adolescents report use of a stimulant illicitly. Various street names for methamphetamine including ice, speed, crystal, glass, and crank. This agent can be used in a host of ways, including injection, inhalation, and smoking. Similar to cocaine, dependence can develop quickly and be associated with a rapid decrement in functioning. Associated effects can include psychotic behavior; aggression; and various neuropsychological deficits, including memory loss. Appetite suppression is common as is decreased need for sleep. Euphoria is often noted. Physical effects include hyperthermia, increased respiration, and increased risk for seizures.
MDMA (3,4-methylenedioxymethamphetamine) (“Ecstasy”) is another frequently abused agent with both stimulant and psychedelic effects. Slightly more than 1% of adolescence report using it over the course of a year. Taken orally, the psychedelic effects of the agent last for several hours. Mental status changes can include anxiety, paranoia, depression, and sleepless. Physical symptoms can include blurred version, a sense of muscle/body tension, nausea, and sweating; occasionally, severe hyperthermia develops. Available data suggest that most users stop use of the agent in young adulthood, although some who become dependent continue.
GHB (γ -hydroxybutyrate) is known on the street as G, grievous bodily harm, or liquid Ecstasy. This drug was originally used as a muscle growth agent and sold in health food stores before its CNS effects were recognized. A CNS depressant, many of the effects of GHB are similar to those of alcohol. Effects last for several hours. Dependence can develop along with a withdrawal syndrome similar to that sometimes seen with benzodiazepines. About 2% of high school seniors report use of this agent in the previous year (Hopfer & Riggs, 2007).
Although many (about one in six) adolescents will have tried inhalants on at least one occasion, actual rates of abuse or dependence are much lower, around 0.1% (Sakai et al., 2004). These organic fumes and gases are more frequently abused in younger adolescents probably because of greater accessibility. These compounds can be sprayed into the mouth or inhaled either through putting the material into a cloth and inhaling it (“huffed”) or by inhaling via a bag (“bagged”). Psychological effects include euphoria and disorientation. A period of drowsiness or confusion may follow. A variety of materials are inhaled. They have the potential for causing relatively rapid neurological features and changes in cognition. Their continued use can lead to neurotoxicity, making detection and treatment important public health problems.
Anabolic steroid abuse has become relatively common, with about 3% of male adolescents in the United States reporting use in the prior year. The main goal for abuse of steroid is building muscle mass, so intrinsically, abuse of these agents differs from other substances of abuse in which the effect has more to do with immediate psychological changes. There are many different medical and psychological sequelae, including stopping growth prematurely and testicular shrinkage. Psychological problems can include pronounced mood swings and even psychosis (Brown, 2005).
EPIDEMIOLOGY AND DEMOGRAPHICS
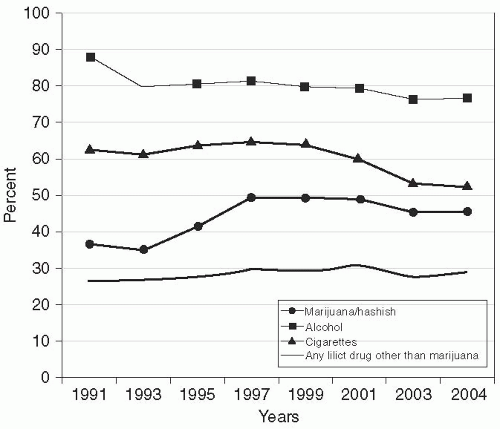
There have been major changes in the use of drugs over the past decade in adolescents in the United States. As noted in Figure 15.1, there have been some fluctuations in patterns of substance abuse, although the most consistently used substances in adolescents have included alcohol, tobacco, and marijuana. About one-third of high school seniors report use of some illegal substance (apart from marijuana) at some point in their lives. Variations in patterns of substance abuse are noteworthy but not always well understood. There has been a noteworthy increase in the use of hydrocodone in adolescents.
Age-related data from publicly funded substance abuse treatment programs are presented in Table 15.1. For younger adolescents, marijuana is most frequently cited as the primary substance of abuse, but for the oldest adolescents and young adults, marijuana combined with alcohol continues to be a major problem along with a variety of other substances. There is a steady increase in prevalence of substance use and disorders of substance use over the course of adolescence with about 25% of older adolescents meeting criteria for abuse and 20% for disorder.
FIGURE 15.1. Trends in prevalence of twelfth grade lifetime drug use. (Adapted from Johnson, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2005). Monitoring the Future: National Survey Results on Drug Use, 1975-2004. Volume 1: Secondary School Students. Bethesda, MD: National Institute on Drug Abuse; 680. NIH Publication No. 05-5727.)
Boys and young men are more likely to engage in substance abuse and also are more likely to meet criteria for dependence in late adolescence, particularly for alcohol and marijuana. Girls and young women are more likely to report nicotine dependence. Rates of substance use disorders are high in a mental health setting and even more so in juvenile justice setting, where a majority of individuals meet lifetime criteria for substance use disorders.
Risk appears to increase with early onset of substance use. It remains unclear why this is so, although animal studies have suggested greater potential for vulnerability to drug sensitization during the adolescent period. It may also be that early use of substances arises as a result of more general risk factors.
ETIOLOGY
Various risk factors are associates with substance abuse disorders in adolescents (see Whitmore & Riggs, 2006). Obviously, development of these disorders depends on ready access to substances of abuse. However, even when these substances are widely available, only a small number of adolescents develop substance use disorders. Attempts have been made to understand genetic and environmental factors using twin and adoption studies. Genetic factors become more apparent if environments support their expression. Genetic mechanisms can be complex (e.g., there may be a direct impact on the ability to metabolize or react to substances). Effects may also be more indirect (e.g., by impacting other aspects of development or behavior). It is clear that family history of substance abuse or dependence is a powerful predictor of risk.
Risk for substance and abuse and dependence is increased in association with a number of other conditions. For example, the various externalizing disorders are a major risk factor (Crowley & Riggs, 1995). Because of their frequent association with each other, disentangling contributions of these conditions is complicated, but it is clear that conduct disorder is a major risk factor and the less severe oppositional defiant disorder (ODD) and even attentiondeficit/hyperactivity disorder (ADHD) also appear to increase risk.
TABLE 15.1 PRIMARY ADMITTING SUBSTANCE OF ABUSE (% OF TOTAL ADMISSIONS), BY AGE FROM THE TREATMENT EPISODE DATA SET
Substance
Age (years)
12-14 %
15-17 %
18-20 %
None
8.3
2.2
0.9
Alcohol
17.7
19.9
30.6
Crack or cocaine
1.2
2.4
6.3
Marijuana or hashish
66.7
66.9
37.9
Heroin
0.2
1.2
9.8
Nonprescription methadone
0
0
0.1
Other opiates and synthetics
0.4
0.6
2.5
PCP
0.1
0.1
0.4
Hallucinogens
0.1
0.3
0.4
Methamphetamine
2.1
4
8.4
Other amphetamines
0.6
0.9
1.4
Other stimulants
0.2
0.1
0.1
Benzodiazepines
0.2
0.2
0.4
Other tranquilizers
0.1
0.1
0
Barbiturates
0
0
0
Other sedatives or hypnotics
0.2
0.1
0.2
Inhalants
0.9
0.2
0.1
Over-the-counter medications
0.2
0.2
0.1
Other
0.9
0.6
0.5
Total percent
100
100
100
(Total N)
(24,911)
(123,496)
(119,138)
PCP, phencyclidine.
From TEDS: Treatment Episode Data Set. (2003). Highlights. National Admissions to Substance Abuse Treatment Services, DASIS Series: S-27. Rockville, MD: Services DoHaH. DHHS Publication No. SMA 05-4043, with permission.
Only gold members can continue reading. Log In or Register to continue