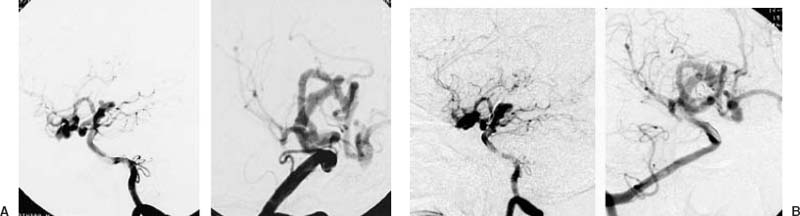
14 Diagnosis High-positioned giant basilar top aneurysm Problems and Tactics A usual modification of the surgical approach for a high-positioned basilar top aneurysm is an addition of the orbitozygomatic osteotomy1,2 to a pterional or sometimes to a subtemporal approach. The approach through the third ventricle via the interhemispheric fissure3 may be applied less frequently in selected cases; however, if the position is extremely high (> 1.5 cm from the level of the top of the posterior clinoid process) and the aneurysm is giant in size, special consideration is required. This case describes such a condition. Keywords Giant basilar top aneurysm, high position, skull base surgery infratemporal approach, clipping A 63-year-old male had a subarachnoid hemorrhage (SAH) 10 years earlier. The examination at that time revealed bilateral occlusion of the internal carotid artery at the neck and circulation of the whole brain was supplied through the vertebrobasilar system through the posterior communicating arteries. The basilar artery was elongated and tortuous. There was a small aneurysm pointing forward at the top of the basilar artery; however, the aneurysm was not treated at that time because of the high position of the basilar bifurcation, 12 mm from the level of the posterior clinoid process. Two years later a second SAH occurred (Fig. 14–1A). At this time clipping of the aneurysm was performed via a right pterional transsylvian approach with an addition of the orbitozygomatic osteotomy. The anterior clinoid process was removed and the right carotid artery that had been occluded was cut at its entry to the intradural space. A Sugita clip (7 mm blade length) was applied (Fig. 14–1B). The patient was free from symptoms postsurgery and was followed up regularly thereafter. It was noticed that the aneurysm had been gradually enlarging, and 8 years after the last operation it ruptured a third time. The aneurysm was 3 cm in diameter. The clip of the previous operation was on the anterior wall of the aneurysm, and the upper dome of the aneurysm reached 23 mm from the level of the posterior clinoid process (Fig. 14–2A, B). Consciousness disturbance with left oculomoter nerve palsy was present. There was a thick cisternal hemorrhage around the top of the basilar artery and hematoma in the third ventricle and the aneurysm was seen as a negative shadow in hematoma in the cistern. Two months later the patient had recovered somewhat, showing recent memory disturbance, left oculomoter nerve palsy with mild right hemiparesis, and trunkal ataxia. To prevent further ruptures and to decompress the brain stem active treatment was considered to be necessary. Endovascular surgery would not be indicated because of the lack of an apparent neck of the aneurysm, and trapping the aneurysm was considered too risky even with installment of a high-flow bypass because the basilar artery supplied blood flow for the whole brain. The direct operation was then considered the sole choice for treatment. FIGURE 14–1
An Extremely High-Positioned Giant Basilar Top Aneurysm Operated via Infratemporal Approach
Clinical Presentation
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


