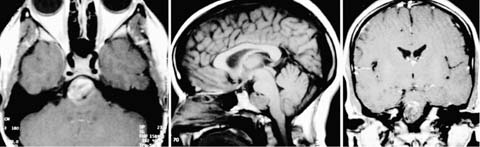
16 Diagnosis A giant midbasilar artery fusiform aneurysm Problems and Tactics In this case we are presenting the case of a young woman with a newly discovered giant midbasilar artery aneurysm. The aneurysm was suspected initially on the basis of computed tomographic (CT) scan, magnetic resonance imaging (MRI), and MR angiogram (MRA) after an acute onset of syncope. The cerebral angiogram confirmed the diagnosis of an unruptured giant midbasilar artery fusiform aneurysm. We discuss the decision-making process and the perioperative management, as well as a detailed description of the surgical technique for cases similar to the one presented here. Keywords Giant mid-basilar fusiform aneurysm, superficial temporal to superior cerebellar artery bypass, distal clipping of the aneurysm This is a 25-year-old, right-handed female and financial analyst. She was in her usual state of health when suddenly she developed a sensation of dizziness and blurry vision at work. She also felt nauseated and lost consciousness for a few minutes. Upon awakening, she had a generalized weakness with urinary incontinence. No seizure activities were witnessed at that time. She subsequently developed pounding occipital headaches. She was taken to a local hospital, where initial CT-scan and MRI/MRA were performed, revealing a large basal lesion suspicious for a large skull base tumor versus a basilar artery aneurysm (Fig. 16–1). There were no signs of subarachnoid hemorrhage. She then underwent a four-vessel cerebral angiogram where an unruptured giant midbasilar artery fusiform aneurysm was found (Fig. 16–2). The aneurysm was partially calcified with mass effect compressing the brain stem. Both posterior cerebral arteries (PCA) were of fetal origin. A small P1 segment was present on the right side only. The anterior inferior cerebellar artery (AICA) was arising from the basilar artery (BA) near or in the area involved by the aneurysmal dilatation. This type of giant fusiform aneurysms are at risk for progressive enlargement and compression of the brain stem, as well as thrombosis causing large brain stem stroke. The risk for rupture increases with the enlargement of the aneurysm. Fusiform aneurysms are generally not good candidates for endovascular coiling. Endovascular stenting may be possible in the future, but an appropriate stent is not available at present. In this case, AICA flow needed to be preserved through the BA. FIGURE 16–1 Initial magnetic resonance imaging at the presentation, showing the lesion. A radial artery graft bypass into the PCA was considered, but this was not thought to be appropriate because of the minuscule P1 segment. Because of this, we selected a superficial temporal artery (STA) to superior cerebellar artery (SCA) bypass. Because it was felt that the aneurysm was thick walled, occlusion of the BA distal to the aneurysm was elected, allowing the flow to continue through the BA into the AICA. The patient was anesthetized and placed in the supine position using a radiolucent head holder, with the head turned 70 degrees to the left side. The course of the right superficial artery was identified by Doppler, and it was dissected using the surgical microscope. A C-shaped incision was started from here and curved retroauricularly (Fig. 16–3). A temporal and transpetrosal craniotomy was then performed. A partial labyrinthectomy petrous apictectomy transpetrosal approach was performed. After a presigmoid and subtemporal approach with the division of the tentorium, the fusiform BA aneurysm was exposed medial to cranial nerves (CN) VII and VIII. The BA distal to the aneurysm was deviated to the contralateral side and was exposed with some difficulty medial to the CN V. The SCA was dissected on the lateral surface of the midbrain (Fig. 16–4), and a 1-cm segment free of perforators was isolated and a small rubber dam placed under it. At this point, the distal end of the STA was prepared by denuding it free from the periadventitial and adventitial tissues. This distal end was obliquely sectioned to create a fishmouth orifice of 3 mm in diameter. Heparinized saline solution was used to flush out the artery blood-free, whereas the proximal temporary clip was opened and closed. The SCA was temporarily occluded after burst suppression was accomplished with barbiturates to protect the brain, and an arteriotomy was created in the SCA. Using 10–0 sutures, an end-to-side anastomosis was performed between the STA and SCA. After removal of the clips, there was excellent flow in the graft and antegrade, using a Doppler probe. The total occlusion time was 55 minutes. Then a Sugita titanium clip No. 16 was used to occlude the basilar artery just beyond the aneurysm (Fig. 16–5) with the idea that the aneurysm would clot off up to the most distal branch, which was the AICA in this case (Fig. 16–6).
Management of a Giant Midbasilar Artery Fusiform Aneurysm
Clinical Presentation
Treatment Strategy
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


