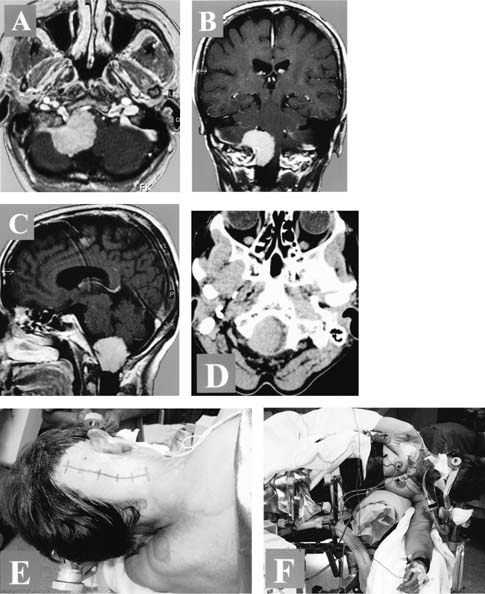
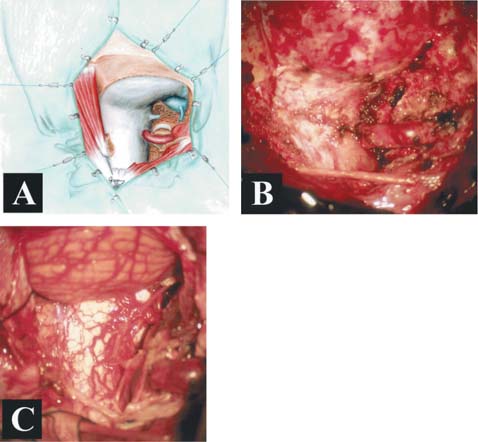
51 Diagnosis Lateral foramen magnum meningioma with severe brain stem compression Problems and Tactics A large meningioma originating from the right jugular tubercle and anterolateral foramen magnum region has caused a severe compression and displacement of the lower brain stem. Considering the location of the tumor and the fact that the intradural vertebral artery (VA) and the caudal cranial nerves were encased by the tumor, a special surgical procedure using the so-called transcondylar approach was designed to allow for safe tumor removal and brain stem decompression with preservation of all caudal cranial nerves and arterial branches of the vertebral artery. Keywords Foramen magnum, jugular tubercle, meningioma, transcondylar approach This 57-year-old female suffered for years from nuchal pain. During the months before surgery she complained of progressive gait disturbance. Neurological examination revealed a moderate gait ataxia but no focal deficits. Computed tomographic (CT) scan and magnetic resonance imaging (MRI) revealed a large right-sided antero-lateral meningioma. The lower brain stem was maximally compressed at the level of the foramen magnum where the tumor occupied more than 90% of the available space (Fig. 51–1). The procedure was performed under general anesthesia with the patient placed in the left lateral position. The head was flexed and rotated to the right side (Fig. 51–1). Continuous monitoring of somatosensory and auditory evoked potentials was applied during surgery. After a slightly curvilinear retroauricular skin incision, the right dorsolateral craniospinal region was exposed including the condylar fossa, the lateral atlantal arch up to the midline, and the horizontal portion of the vertebral artery, which extended posteriorly beyond the level of the C1 arch. A lateral suboccipital craniotomy extending to the distal sigmoid sinus and a C1 hemilaminectomy were perfomed and the dorsolateral rim of the foramen magnum was gradually drilled away paying great care to the underlying brain stem and spinal cord. To reach the anterolateral rim of the foramen magnum near the level of the hypoglossal canal, the medial portions of the lateral atlantal mass and of the occipital condyle were drilled away together with the dorsal portion of the jugular tubercle. This area corresponded to the main region of dural attachment of the meningioma. The entrance point of the vertebral artery into the dura mater was completely dissected free not only medially but also laterally, to allow for a sufficiently lateral viewing direction. A diamond burr was used for drilling, and this step of the procedure was undertaken with great care for the medial portion of the jugular bulb and vertebral artery (Fig. 51–2). The dura was opened medial to the vertebral artery close to the dural ring, reflected laterally together with the artery itself, and fixed with temporary sutures. Direct access to a highly vascularized meningioma and particularly to the dural attachment of this tumor became available. FIGURE 51–1 (A) Axial, (B) coronal, and (C) sagittal magnetic resonance imaging and (D) computed tomographic scan at the level of the foramen magnum obtained before surgery. (E) Skin incision and (F) positioning of the patient during surgery. FIGURE 51–2 (A) Illustration showing the dural exposure of the right dorsolateral craniospinal region; after craniotomy and C1 hemilaminectomy, a partial resection of the jugular tubercle, the occipital condyle, and the lateral atlantal mass have been performed. (B) Intraoperative photograph showing the same exposure. (C) The intradural site after tumor removal.
Large Meningioma of the Jugular Tubercle and Foramen Magnum
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


