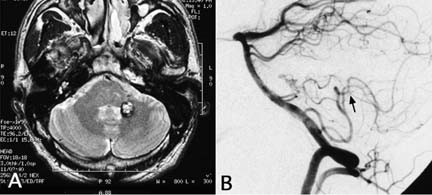
60 Diagnosis Cavernous hemangioma in the brachium pontis Problem and tactics A cavernous hemangioma located in the inferomedial part of the brachium pontis was resected with a transcerebellomedullary fissure (CMF) approach.1 During the surgery, it was difficult to open the fissure to a sufficient width due to the anatomy of the posterior inferior cerebellar artery (PICA). The lesion was accessed via a lateral recess. Keywords Brachium pontis, cavernous hemangioma, transcerebellomedullary fissure approach A 44-year-old man presented with sudden onset of gait disturbance and a floating sensation, which had improved for 10 days. On admission 4 months after onset, no neurological deficit was apparent. Magnetic resonance imaging (MRI) revealed a cavernous hemangioma surrounded by hemosiderin-laden brain in the inferomedial portion of the cerebellar peduncle on the left side. The lesion was close to the ependymal surfaces at the lateral wall of the fourth ventricle and lateral recess. Left vertebral angiography showed that the bifurcation of the vermian and tonsillohemispheric branches of the posterior inferior cerebellar artery (PICA) was located distal to the cranial loop (Fig. 60–1). The patient was placed in the semiprone park-bench position on the right side with the head maximally flexed. After standard midline suboccipital craniotomy with C1 laminectomy, the posterior fossa dura was opened with a Y-shaped incision extending toward the level of the axis. The tonsil was dissected away from the uvula and medulla oblongata on the left side. The bifurcation of the vermian and tonsillohemispheric branches distal to the choroidal branches was located on the posterior medullary velum, and multiple small branches led off from the posterior medullary segment of the left PICA close to the taenia. Dissection of the cranial loop of the PICA from the pial surfaces was therefore thought to be excessively dangerous, preventing the wide opening of the fourth ventricle from the foramen Magendie to the foramen Luschka. Even if this could be achieved without arterial damage, the bifurcation of the vermian and tonsillomedullary branches would necessarily have been in the center of the route to the lesion, impairing direct observation of the lesion and at risk of being damaged. A subtonsillar approach via the lateral recess, laterally to the cranial loop of the PICA, was used to access the lesion. After retracting the tonsil upward, the lateral recess was fully opened by dissecting the tela choroidea laterally to the foramen Luschka (Fig. 60–2A). The dark-colored roof of the lateral recess was incised in linear fashion using a round knife (Fig. 60–2B). A relatively large intraparenchymal vein, running transversely and receiving a vein from the lesion site, was first exposed (Fig. 60–2C). The hemangioma was carefully and meticulously dissected from the gliotic neural tissue and resected piecemeal (Fig. 60–2D). To expose the dorsal surface of the lesion, the axis of the microscope (Super OH/MM-2; Mitaka, Tokyo) was turned dorsally as much as possible. In addition, the tonsil had to be significantly retracted. By these means, total removal of the lesion was accomplished under direct vision, preserving the vein adjacent to the lesion (Fig. 60–2E,F). FIGURE 60–1 Preoperative images. (A) Axial T2-weighted magnetic resonance imaging showing a cavernous hemangioma in the left cerebellar peduncle. (B)
A Case of Cavernous Hemangioma in the Brachium Pontis
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


