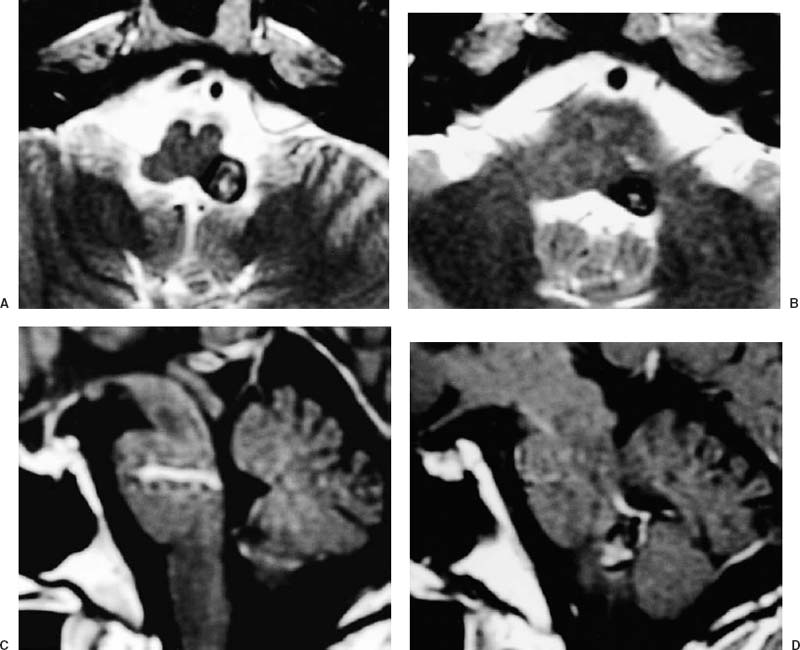
61 Diagnosis Cavernous angioma in the medulla oblongata associated with venous angioma in the pons Problems and Tactics A cavernous angioma in the posterolateral side of the medulla oblongata was associated with a venous angioma in the pons. Because the patient suffered from repeated hemorrhages, surgical resection of the cavernous angioma was required while leaving the venous angioma intact. Keywords Cavernous angioma, venous angioma, medulla oblongata, surgery This 49-year-old man suffered headaches, dysarthria, and dysphagia, and was found to have a hemorrhagic cavernous angioma in the left medulla oblongata on computed tomography (CT) and magnetic resonance imaging (MRI). He was initially treated conservatively, but repeated bleeding occurred over a 2-year period, and the patient had transient neurological deficits, including left facial weakness, and dysphagia. The latest MRI and angiography indicated that the cavernous angioma was located slightly caudal to the venous angioma (Figs. 61–1, 61–2). A direct surgery of the cavernous angioma was therefore thought to be feasible. He had no apparent neurological deficits preoperatively, except for mild dysarthria and left facial weakness. Under general anesthesia, the patient was placed prone1 with his head flexed and fixed in a head frame. A midline suboccipital approach was made with a linear skin incision. The foramen magnum was opened and then the dura mater was opened in a Y-shaped manner down to just above the C1 laminae. An operating microscope was positioned and the surgeon operated on the patient from the patient’s left caudal side. The cisterna magna was opened, and the bilateral tonsils were visualized. Retracting each tonsil laterally, the obex and the lower part of the floor of the fourth ventricle were exposed. The left cerebellomedullary fissure was opened, and the floor of the fourth ventricle and left gracile tubercle were further exposed. The left lower part of the floor of the fourth ventricle was yellowish, but no hematoma was visible (Fig. 61–3). Before incising the abnormal-looking ventricular floor, brain stem mapping was performed to identify the location of the facial nucleus. Because no positive responses were obtained from the abnormal-looking area, it was incised longitudinally 6 mm lateral to the median raphe. Within 1 to 2 mm, the hematoma cavity was entered. An old clot was evacuated with a thin suction tube, and the surface of the angioma appeared. The margin of the angioma was identified and dissection proceeded in the surgical plane. A small cotton sheet was placed on the margin of the dissection to protect the pontine parenchyma, and the angioma was dissected using a cotton-wiping method; the surface of the angioma was wiped away from the surrounding structures using a small, thin, cotton sheet, Bemsheet® (Osaka Kogyo Ltd. Co., Osaka, Japan). Fibrous structures and vascular connections were cut with microscissors. Inferomedially, the angioma was thin-walled, bulged, and vascular rich. This part of the angioma was coagulated to shrink it, and was dissescted from the surrounding structure to minimize retraction of the pons. There was a clear cleavage line between the parenchyma of the pons and the angioma; a hemosiderin layer was present. The angioma was then dissected and totally removed. Complete dissection was achieved with a 6-mm long incision on the floor of the fourth ventricle. No abnormal vessels were encountered in the venous angioma during this procedure. The dura mater was closed and the wound was closed in the standard manner. FIGURE 61–1 (A,B)
Cavernous Angioma in the Medulla Oblongata Associated with Venous Malformation
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


