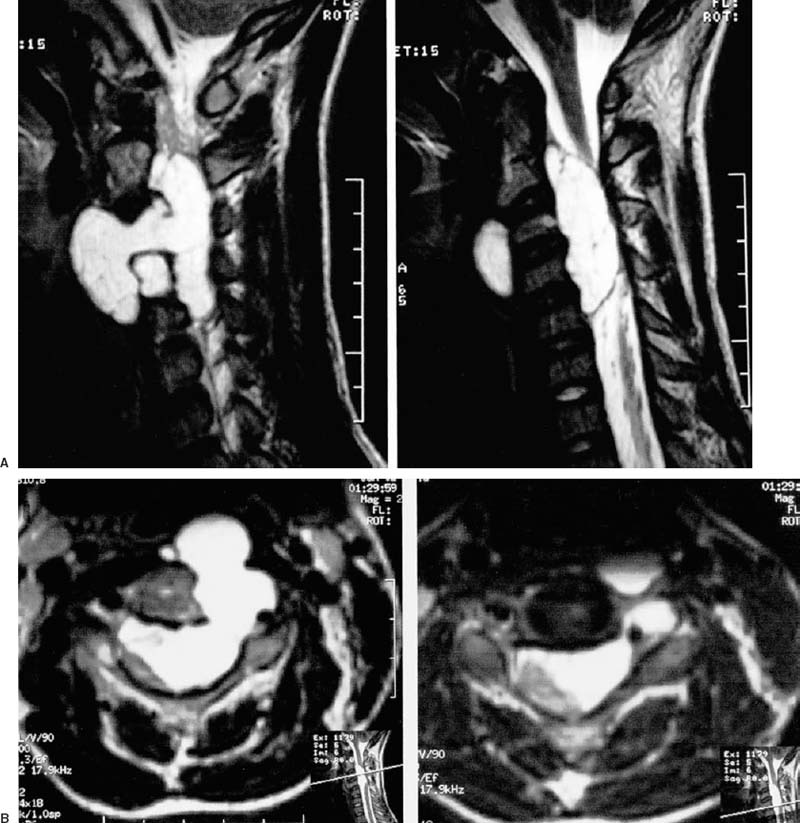
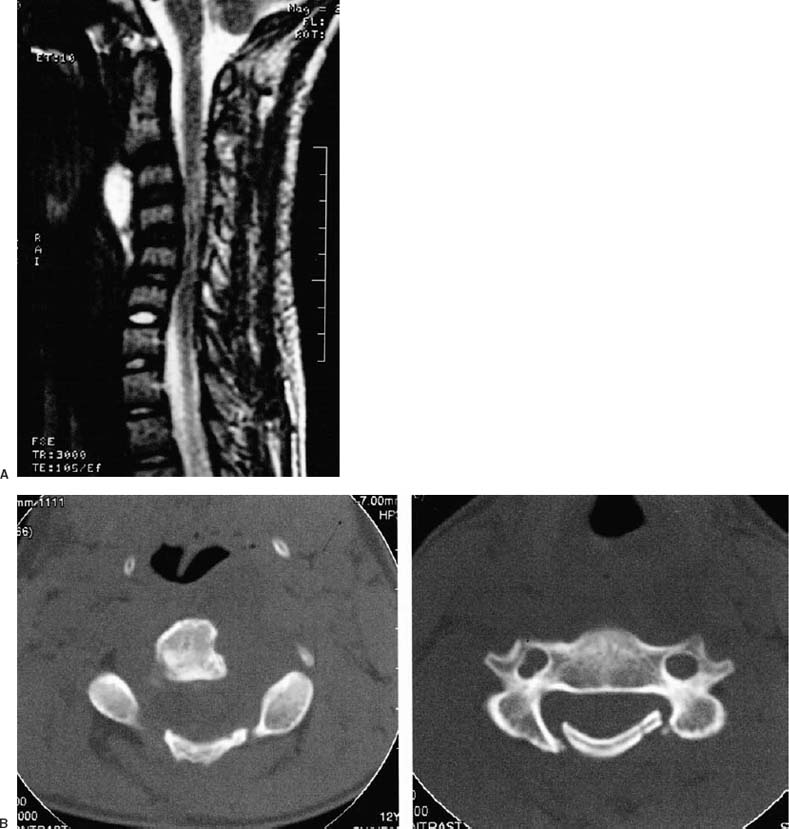
65 Diagnosis Pediatric cervical spine chordoma Problems and Tactics A complex pediatric upper cervical dumbbell chordoma presented with severe spinal cord compression and engulfed the vertebral artery breaking into the retropharyngeal space. Dorsal cervical cord decompression with osteoplastic laminectomy relieved the cord compression but new neurological symptoms arose. Instability, complicated with the sinking in of laminoplasty and the need for gross-total resection led to two surgical procedures to give the best result. Keywords Pediatric vertebral tumors, cervical chordomas, spinal cord compression This 11-year-old boy had neck pain, occipital headaches, and left arm weakness of 6 weeks’ duration. A huge intradural and extradural spinal chordoma was visualized on magnetic resonance imaging (MRI) with cervical cord compression to the right and tumor extending through the lateral aspect of the C3 and C4 vertebral bodies, engulfing the left vertebral artery and also presenting retropharyngeally (Fig. 65–1A,B). The patient underwent C2–C5 laminectomy for tumor within the spinal canal and the osteoplastic laminectomy was sutured in place. The patient had no left biceps and deltoid function postoperatively with absent pain sensation in the C5 and C6 distributions on the left. He had improvement in his quadriparesis. Severe left arm pain required narcotic analgesics. He presented to us for further care. MRI revealed midcervical kyphosis and relief of the spinal cord compression but with enhancement in the lateral gutters within the spinal canal (Fig. 65–2A). Thin-section cervical spine computed tomography (CT) demonstrated the ventrally migrated osteoplastic laminectomy with encroachment into the neural foramen on the left side (Fig. 65–2B). There was tumor in the neural foramen engulfing the vertebral artery and tumor replacing the left half of the C3 and C4 vertebral bodies. Selective vertebral angiography identified the major feeders to the tumor and these were embolized. The patient tolerated test occlusion of the left vertebral artery, which was likewise engulfed with tumor (Fig. 65–3). Crown halo cervical traction at 7 lbs was applied with sedation, and somatosensory evoked responses were unchanged. Nasal endotracheal general anesthesia ensued, and the patient was positioned prone and fixated with cervical traction in place. The posterior cervical incision was reopened. The laminae at C4 and C5 had “dropped” into the spinal canal. There was instability between C3 and C5. Significant adhesions were encountered between the spinal cord and the dura, as well as among the nerve roots. Neurolysis was accomplished on the left between the C4–C6 roots. There was good contraction obtained of the deltoid as well as the biceps with stimulation of the C5 and C6 nerve roots. The laminae were replaced and fixated with a miniplate system. A right lateral mass fusion between C3 and C6 was made using facet screws and a lateral mass plate. The patient’s biceps and left deltoid function recovered over the next few days and his arm pain subsided. FIGURE 65–1 Composites of T2-weighted magnetic resonance imaging in (A) sagittal and parasagittal and (B) axial planes at the level of the C3 and C4 vertebral bodies. The chordoma fills the spinal canal with gross compression of the spinal cord to the dorsal right of the midline. The tumor proceeds through the left lateral aspect of the C3 vertebral body, engulfing the left vertebral artery to present in the retropharyngeal space. FIGURE 65–2 (A) Midsagittal T2-weighted magnetic resonance imaging of the cervical spine made after the initial operative intervention. Note the midcervical kyphosis and canal stenosis with residual tumor anteriorly. (B)
A Case of Complex Chordoma of the Mid and Upper Cervical Spine in an 11-Year-Old
Clinical Presentation
Surgical Technique
First Operation
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


