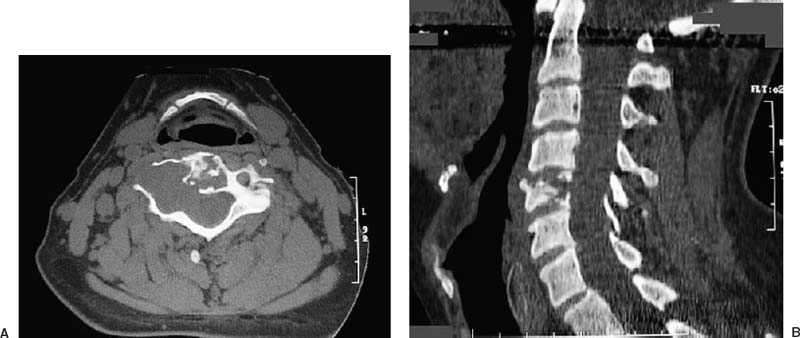
66 Diagnosis Schwannoma Problems and Tactics Extensive bony destruction of the cervical vertebrae at C5 was identified after a man fell 20 feet. Further evaluation revealed an intradural–extradural tumor encasing the vertebral artery. Surgery was planned in two stages for tumor resection and anteroposterior reconstruction of the cervical spine. Keywords Schwannoma, cervical spine, lateral mass plates, corpectomy, instrumentation A healthy 51-year-old man fell 20 feet off a ladder and immediately experienced neck pain radiating to his right shoulder. He was admitted through the trauma service, where radiographs revealed a C5 compression fracture. Computed tomography (CT) confirmed the fracture with bone remodeling and an enlarged C4–C5 neural foramen (Fig. 66–1). Magnetic resonance imaging (MRI) revealed a very large cervical tumor extending from C3 to C5 and exiting through the right C4–C5 neural foramen. The tumor involved both the intradural and the extradural compartments (Fig. 66–2). Angiography was performed to assess the involvement of the vertebral artery. The patient was placed in the prone position in the Mayfield headholder (Codman, Inc., Raynham, MA). Somatosensory evoked potentials (SSEPs) recorded before and after positioning showed no changes. The patient’s cervical spine was placed in a neutral position under fluoroscopic guidance. A midline posterior cervical incision was carried down to the spinous processes. Fluoroscopy was used to confirm the appropriate levels. Subperiosteal dissection continued over the lamina and to the lateral extent of the lateral masses from C3 to C7. The point 1 mm medial to the absolute midpoint of the lateral masses was marked, followed by decortication with an awl for later placement of the lateral mass screw. The Anspach M8 drill bit (Anspach, Palm Beach Gardens, FL) was used for a bilateral C3–C5 laminectomy. There was evidence of the extradural component of the tumor and its extension to the lateral mass plates. On the right, the C4–C5 facet was loose and floating, and the pedicle was eroded anteriorly by the tumor. The right C4–C5 facet and inferior aspect of the C3 facet were resected to maximize the exposure. After hemostasis was achieved, the microscope was brought into the operative field. The extent of the lesion was delineated, and a significant intradural portion was noted. A midline durotomy performed with a blade was extended with a dental tool. The dura was tented to protect the neural elements from the blade. When the dura was opened, several nerve roots were intimately involved with the tumor, particularly the sensory nerve root of C5. A yellowish, fatty tumor was consistent with a schwannoma or neurofibroma. The dissection plane was developed between the exiting nerve roots and spinal cord, and the tumor was gently dissected. The tumor was freed from the neural elements without retracting the latter and placed in continuity with the large mass laterally. The tumor was then bipolar cauterized along its longitudinal axis and opened with a blade in a longitudinal fashion. A biopsy specimen was consistent with a nerve sheath tumor. FIGURE 66–1 (A) Preoperative axial and (B) sagittal cervical computed tomographic scans show destruction and erosion of the C5 vertebral body with involvement of the posterior elements. On the right, the eroded and expanded neural foramen is impressive. The tumor was debulked in a piecemeal fashion from within, working inside the tumor capsule. The center portion was debulked to a thin rim of tumor and capsule and further dissected from the spinal cord, which was severely indented. In this fashion, the medial bulk of the tumor was dissected along its rostral and caudal extents. When the tumor was mobilized laterally, extensive bleeding from the epidural venous plexus was encountered. The bleeding was controlled with Avitene® (MecChem, Woburn, MA) and pressure was applied with patties.
Intraosseous Tumor of the Cervical Spine
Clinical Presentation
Surgical Technique
Related posts:
 3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
43 Supraorbital Keyhole Craniotomy for Frontobasal Meningiomas
49 Radical Total Resection of a Giant Petroclival Meningioma
3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
43 Supraorbital Keyhole Craniotomy for Frontobasal Meningiomas
49 Radical Total Resection of a Giant Petroclival Meningioma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


