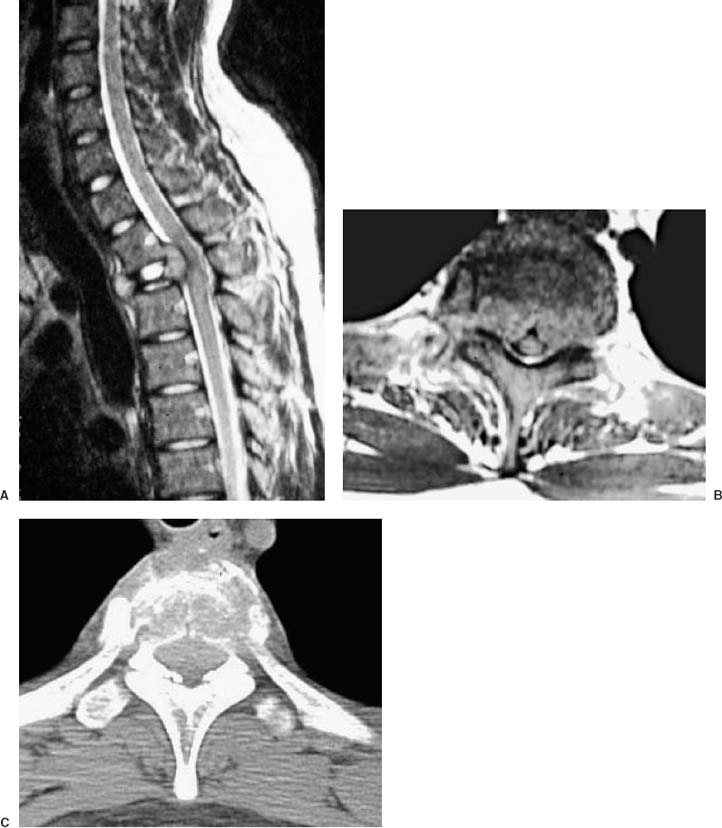
67 Diagnosis Giant cell sarcoma of the Th2 vertebral body Problems and Tactics Primary or metastatic tumors of the spinal column most frequently arise from the vertebral body or the pedicles. For effective treatment, thorough resection from the anterior column, adequate decompression of the spinal cord, and stabilization are necessary. To access tumors arising in the vertebral body of the thoracic spine, various approaches such as thoracotomy or transmanubrium, or lateral extracavitary approaches can be chosen. Modified costotransversectomy combined with transpedicular removal of the vertebral body1 provides a less invasive pathway for the objectives. The approach has an advantage when dealing with a high thoracic lesion because it allows application of instrumentation extending into the cervical segments. In the following case, the nature of the lesion destructing the vertebrae was initially unknown, and in addition to the urgent need of restoring the functional status of this young patient, surgery was indicated to establish the histological diagnosis and appropriate treatment plan. Keywords Total vertebrectomy, transpedicular approach, giant cell sarcoma, pedicle screw fixation, sublaminal wiring This 19-year-old male, who initially complained of intrascapular back pain 4 weeks prior to transfer to our department, developed progressive paraparesis over 2 weeks and became unable to walk. When admitted to a local hospital, he could not raise his thighs or legs against gravity, and had difficulty in urination. Both superficial and deep sensation in the legs were diminished. Magnetic resonance imaging (MRI) and radiological examinations revealed an osteolytic mass arising from the Th2 body, which was largely destructed and collapsed (Fig. 67–1). An emergency laminectomy was performed, but with little improvement in the motor function postoperatively. Pathological examination of the tissue specimen revealed a neoplastic lesion compatible with sarcoma. When he was transferred to our service 2 weeks later, he did not have voluntary movement of the lower extremities, but showed some reflex withdrawal upon stimulation. MRI revealed angulation and a focal impingement of the cord by the tumor located ventrally, with little efficacy of decompression by the laminectomy. The findings, together with the poor functional recovery, which is not unexpected after laminectomy for ventrally located lesions, warranted a radical procedure to remove the mass and reconstruct the spine. FIGURE 67–1 Preoperative magnetic resonance imaging (A,B) and computed tomographic scan (C) showing the osteolytic lesion destructing the Th2 vertebral body and compressing the spinal cord. The patient was placed in a prone position with a neutral alignment of the cervical and thoracic spine, and with the head fixed by a Mayfield clamp. The previous wound for laminectomy (Th1,2,3,4) was opened in the midline. Exposure was extended to C6 to Th6 for reconstruction with instrumentation including the segments above and below the lesion. The Th2 costotransverse process was removed bilaterally along with the rib heads (5 cm). Care was taken not to cause a tear on the pleura. The vertebral body was entered from the dorsolateral working space through the pedicles in an angle oriented anteromedially (Fig. 67–2
Osteolytic Tumor of the Th2 Vertebral Body, Causing Progressive Paraparesis in a 19-Year-Old
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 62 Intramedullary Spinal Arteriovenous Malformation
62 Intramedullary Spinal Arteriovenous Malformation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


