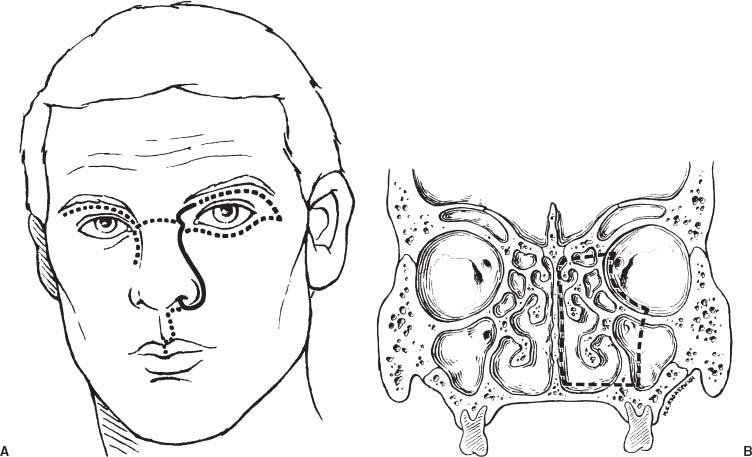
70 Diagnosis Fibrous dysplasia involving the left nasal cavity, nasoethmoidal complex, and sphenoid sinus Problems and Tactics An otherwise healthy 8-year-old girl presented with a 3-year history of progressive left nasal obstruction and headache, leading to the diagnosis of fibrous dysplasia involving the left nasal cavity, nasoethmoidal complex, and sphenoid sinus. Despite the challenges associated with surgery of the pediatric skull base, a craniofacial resection was undertaken in light of the patient’s progressive functional impairment. Keywords Fibrous dysplasia, skull base, pediatric, craniofacial resection This previously healthy 8-year-old girl presented with a 3-year history of progressive left nasal obstruction associated with headache. Physical examination revealed the presence of anosmia, but no other neurological deficit. Formal ophthalmological evaluation confirmed the absence of any significant functional compromise of the optic nerves. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed the presence of a large cystic and solid expansile mass based within the left nasoethmoidal complex and sphenoid bone. The mass greatly expanded the left nasal cavity with consequent bowing of the nasal septum to the right. A slight degree of narrowing of the left optic canal and inferior orbital fissure was also observed. The imaging diagnosis was consistent with fibrous dysplasia involving the paranasal sinuses and anterior skull base. The patient was placed supine on the operating table and orotracheally intubated. Prophylactic intravenous antibiotics with broad spectrum activity against nasopharyngeal flora were administered. A temporary tarsorraphy was placed in both eyes to provide corneal protection during the procedure. The patient was prepared for a bicoronal scalp flap and a bifrontal craniotomy should an intracranial approach be needed to supplement the transfacial resection. If required, we were also prepared to harvest a broad-based, apron-shaped vascularized pericranial flap in the event that it would be required for reconstruction of the anterior fossa floor. The operation began with the transfacial resection via a lateral rhinotomy/medial maxillotomy approach (Fig. 70–1A). An incision was made beginning just under the medial aspect of the eyebrow, slightly medial to the supraorbital notch. The incision was carried inferiorly between the medial canthus and the nasal dorsum, along the nasomaxillary junction, around the alar crease and into the nasal vestibule. The flaps were then elevated. The periosteum was incised and elevated to expose the medial orbital wall and the anterior maxillary wall as far inferior as the piriform aperture and as far laterally as the infraorbital foramen. A low nasal bone osteotomy followed by a medial nasal bone osteotomy was then performed to allow the nasal skeleton and associated soft tissues to be reflected and retracted medially (Fig. 70–1). The medial orbital periosteum was elevated, and the periorbita retracted laterally. The medial canthal tendon was separated from the lacrimal crest, elevated in a subperiosteal fashion, and also retracted laterally with the remainder of the periorbita. The lacrimal sac was mobilized from the lacrimal fossa and the lacrimal duct transected to facilitate lateral displacement of the orbital contents. FIGURE 70–1 (A) Planned surgical incision for a lateral rhinotomy/medial maxillotomy approach to an anterior cranial base tumor (solid line). This incision can be extended (dotted lines) to provide access to laterally situated structures in the midface. (B) Extent of osteotomies within walls of ethmoid and maxillary sinuses to allow for optimum exposure of the tumor (hatched line). Retraction of the periorbita allowed visualization of the anterior and posterior ethmoidal arteries lying along the frontoethmoidal suture line. These vessels were cauterized and divided. The lamina papyracea was taken down to expose the superomedial portion of the tumor. Osteotomies were then created to perform medial maxillotomy and resection of the entire ethmoidal complex on the side of the lesion (Fig. 70–1B
Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Clinical Presentation
Surgical Technique
Related posts:
 3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
43 Supraorbital Keyhole Craniotomy for Frontobasal Meningiomas
49 Radical Total Resection of a Giant Petroclival Meningioma
3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
43 Supraorbital Keyhole Craniotomy for Frontobasal Meningiomas
49 Radical Total Resection of a Giant Petroclival Meningioma
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


