A New Approach to Lumbar Disc Prosthesis
J. P. Steib
Spine surgery is the little sister of orthopaedic surgery. In the last century, we saw limb surgery advance with arthrodeses then osteotomies of the hip and knee held by plaster and then by osteosynthesis. Prostheses were a natural progression, first for the hip and then the knee. After a few years of trial and error these prostheses became firmly established as the gold standard of surgery, causing indications for arthrodesis to disappear and indications for osteotomies to decrease dramatically. But there are only two hips and two knees, whereas there are five lumbar stages and at each level there are three joints providing six degrees of freedom: flexion-extension, right and left tilt, and right and left rotation.
Ontogenic evolution has made us leave behind the global kyphosis of the baby to achieve cervical and then lumbar lordosis (1). Lordoses are sectors of mobility, and areas in kyphosis are hypomobile. Lumbar lordosis makes walking possible and ensures the anteroposterior balance of the spine. The mobility of a lumbar segment (two vertebrae, a disc, and the soft parts) is achieved on three axes, permitting rotation (3): a horizontal frontal axis for flexion-extension, a horizontal but sagittal axis for right and left tilt, and finally a vertical axis for axial rotation. These movements are checked by the soft parts, which are opposed and guided by the joints that, through their shape, impose the axis of rotation. Modern tools (computer software, finite-element analyses) have shown that the centers of rotation are not single but are dispersed over an area [scatter of points = instantaneous centers of rotation (ICR), the mean of which gives the mean center of rotation (MCR)]. For flexion-extension, the MCR is slightly below the upper vertebral end plate of the lower vertebra, on the posterior third of the vertebra. In flexion a more anterior MCR leads to posterior stretching, an excessively posterior MCR leads to bumping of the anterior corners of the vertebral bodies, and finally an excessively inferior MCR implies severe antelisthesis. Because of the truncated shape of the posterior joints (4), axial rotation is achieved around a posterior vertical axis situated on the spinous process. Each rotation is accompanied by translation of the intervertebral disc (Fig. 21.1), which permits but also checks this movement. The same posterior joints are
responsible for changes in the ICR in the sectors of mobility and impose translation at each movement. These notions of mobile ICR and translation must be taken into account in prosthesis design.
responsible for changes in the ICR in the sectors of mobility and impose translation at each movement. These notions of mobile ICR and translation must be taken into account in prosthesis design.
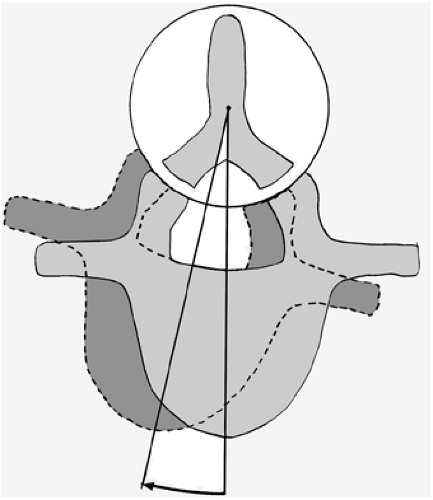 FIGURE 21.1 Translation and rotation. |
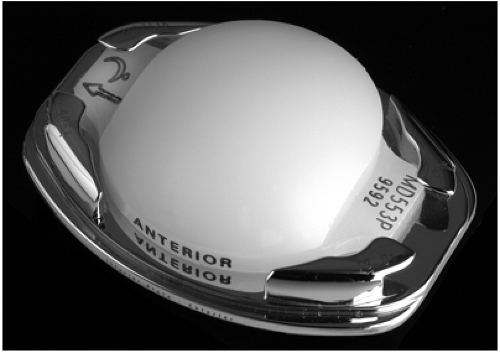 FIGURE 21.2 Mobile core. |
Currently there are semiconstrained disc prostheses (5) with a single set center of rotation that is close to the MCR of flexion-extension. The first prosthesis to be implanted in the world, which has been used for 20 years, is the Charité (6), a nonconstrained prosthesis. This prosthesis with biconvex core has two axes of rotation (upper and lower) that permit an interesting combination of movements to try to adapt to the play of the rear joints. The Mobidisc is a new prosthesis that takes into account the biomechanical study of lumbar intervertebral movement. Like current traditional prostheses, it has a posterior and inferior MCR, but translation of the polyethylene core increases the ICR possibilities (Fig. 21.2). This prosthesis was developed by a group of surgeons: J. Allain, M. Ameil, J. Beaurains, H. Chataignier, J. Delecrin, J. Huppert, M. Gau, M. Onimus, J.-P. Steib, and W. Zeegers. The translation mobility of the polyethylene core on the horizontal plane enables it to adapt to the CRI, which reduces posterior articular stress, wear on the implant, and constraints on the bone-prosthesis interface. The core can center itself on the inferior vertebral endplate by translation and rotation, which assists the relationship between the two vertebrae and forgives an imperfectly median implantation. The prosthesis consists of two endplates, an upper and a lower one, and a polyethylene core. The endplates (three dimensions: 29/24, 34/27, 39/29) are of a truncated elliptical shape. They are made of cobalt-chromium. The surface in contact with the bone is titanium plasma spray coated to facilitate bone integration. An angle-adjustable keel permits primary fixation. Its orientation permits conventional or oblique anteroposterior placement. The lower surface of the upper endplate is concave to fit the convex shape of the polyethylene core. The upper surface of the lower endplate is flat and has four pegs containing the polyethylene and limiting its mobility. There are three versions of the lower endplate: 0-, 5-, and 10-degrees lordosis. The polyethylene core (ultrahigh molecular weight polyethylene) has a flat base and dome-shaped peak 15 mm in diameter. This dome may be median or lateralized backward to bring the MCR further back. Two lateral feet or wings on the right and left fit between the pegs of the bottom endplate. Dislocation of the core is impossible. Its dimensions adapt widthwise to the size of the chosen prosthesis and heightwise to the intersomatic space. Different heights of the polyethylene (6 to 11 mm) determine the prosthesis height of 10, 12, or 14 mm. The endplates-polyethylene core assembly permits all the physiologic movements of a normal intervertebral disc. On the bottom endplate, the core has a mobility of 1.5 mm in all directions. In flexion-extension, the core moves forward and backward and its mobility is ±12 degrees. In lateral tilt, the core moves to the right and left and its mobility is ±10 degrees. In rotation, the core rotates ±6 degrees and shifts to the right and left to follow the translation.
Related posts:
 Adjacent Level Disc Biomechanics
Adjacent Level Disc Biomechanics
 Nucleus Pulposus Regeneration: Present Limitations and Future Opportunities
Nucleus Pulposus Regeneration: Present Limitations and Future Opportunities
 Prosthetic Disc Nucleus: Treatment with the Anterior Approach
Prosthetic Disc Nucleus: Treatment with the Anterior Approach
 Total Lumbar Disc Arthroplasty: Overview of Clinical Results for Existing Implants
Total Lumbar Disc Arthroplasty: Overview of Clinical Results for Existing Implants
 Motion Preservation—Disc Replacement for Lumbar Degenerative Disorders with the ProDisc®-L Prosthesis
Motion Preservation—Disc Replacement for Lumbar Degenerative Disorders with the ProDisc®-L Prosthesis
 Posterior Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Posterior Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


