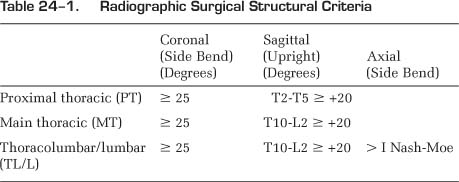
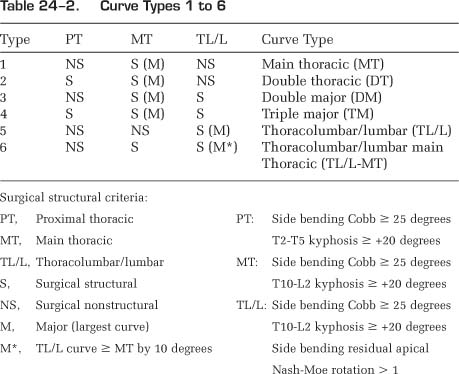
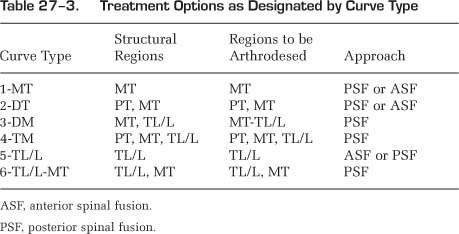
24 A New Classification System of Adolescent Idiopathic Scoliosis 1. To be comprehensive with all types of adolescent idiopathic scoliosis (AIS) curves classified 2. To be two dimensional with applicability to three-dimensional assessment 3. To be treatment based 4. To separate out specific curve types by objective radiographic criteria 5. To be highly reliable 6. To be logical, easily understood, and useful to scoliosis surgeons 1. Curve type 2. Lumbar spine modifier 3. Sagittal thoracic modifier Each of these three components should be identified separately, and then combined together to create the complete classification. Classification begins by reviewing the long cassette upright posteroanterior (PA) and lateral radiographs as well as right- and left-side bending radiographs. The spinal columns are divided into three regions: proximal thoracic (PT), main thoracic (MT), and thoracolumbar/lumbar (TL/L). One must also keep in mind the regional apices of curve designation with a main thoracic apex being located between the body of T2 inclusive to the T11-T12 disc; thoracolumbar curves having apices from the body of T12 to the body of L1 including the T12-L1 disc; and lumbar curves having apices extending from the L1-L2 disc to the body of L4 inclusive. Regional curves are separated into major (largest Cobb) and minor curves. Specific objective criteria in the coronal and sagittal planes determine whether the minor curves are structural or nonstructural. Structural criteria in the coronal plane include inflexibility on side bending ≥ 25 degrees; in the sagittal plane, proximal thoracic (T2-T5) and thoracolumbar (T10-L2) kyphosis ≥ +20 degrees (Table 24–1). Thus, each region of the spine—the PT, MT, and TL/L—is designated as either structural or nonstructural based on these criteria. The largest Cobb measurement is considered the major curve and thus is always structural in these operative cases. A template can thus be created whereby six curve types are designated: type 1—main thoracic; type 2—double thoracic; type 3—double major; type 4—triple major; type 5—thoracolumbar/lumbar; and type 6—thoracolumbar/lumbar—main thoracic (Table 24–2). For curve types 5 and 6, the thoracolumbar/lumbar component should always be a larger Cobb measurement. These curve type designations are treatment-based, for by and large the regions of the spine that are designated structural will require instrumentation and fusion, whereas those nonstructural regions will not. Thus, although not directly providing fusion levels, the curve type designation does implicate appropriate regions of the spine to be included in the instrumentation and fusion, and those regions that should be left unfused (Table 24–3). The lumbar spine is a mobile region of the spine and serves as the foundation of the spine and pelvis. The degree of lumbar deformity is an important determinant of spinal balance and success with scoliosis instrumentation and fusion. Therefore, we have included a lumbar spine modifier to classify the severity of the lumbar deformity in each scoliosis curve and to complement the specific curve types 1 to 6. Lumbar spine modifiers, A, B, and C, are based on the relationship of the center sacral vertical line (CSVL) to the lumbar spine on long cassette upright radiographs. For the lumbar spine modifier A, the CSVL lies between the lumbar pedicles up to the stable vertebra. The curve must have a thoracic apex (curve type 1–4), which excludes any thoracolumbar or lumbar curves (types 5 and 6) (Fig. 24–1). For lumbar modifier B, a major thoracic curve also exists, but the CSVL falls on the apex of the lumbar spine between the medial border of the lumbar concave pedicle and the concave lateral margin of the apical vertebral body or bodies (if the apex is a disc) because of the lateral deviation from the midline of the lumbar spine (Fig. 24–2). And for the lumbar modifier C, the CSVL falls completely medial to the concave lateral aspect of the thoracolumbar/lumbar apical vertebral body or bodies (if the apex is a disc). Thus, lumbar modifier C may exist with any of the curve types 1 to 6, with curve types 5 and 6 always having lumbar curve modifier C because of the necessary deviation from the midline of the apex of the major thoracolumbar/lumbar curve for the curve type 5 and 6 designation in operative cases (Fig. 24–3).
Goals of Surgical Treatment
Curve Classification Triad
Curve Types 1 to 6
Lumbar Spine Modifier
Sagittal Thoracic Modifier (–, N, +)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


