Acquired Disorders of Swallowing, Cognition, Speech, and Language in the Older Adult
Acquired Disorders of Swallowing, Cognition, Speech, and Language in the Older Adult
Karen T. McNett
Alice P. Armbruster
It is the coalescence of remediation and compensation along with providing counseling, education, and information that comprises treatment for acquired dysphagia, cognitive-linguistic, speech, and/or language impairment. The effectiveness of treatment is dependent upon accurate diagnosis. Therefore, this chapter will discuss and provide an overview of various diagnostic and treatment approaches used by the medical speech-language pathologist for acquired disorders of swallowing, cognition, speech, and language in the older adult.
Accurate diagnosis is dependent upon the education, knowledge, and experience of the clinician, use of appropriate diagnostic tools that are valid and reliable, an understanding of normal versus abnormal, and knowledge of the differences between “normal limits” and “functional limits.” Furthermore, delineating strengths and weaknesses in a hierarchical fashion is helpful in developing a plan of action that takes into consideration the patient’s desires and those of his or her family and caregivers. The ultimate objective of therapy is to return a patient to the highest level of function with the least amount of support possible.
Obtaining objective and standardized data will help delineate specific deficits relative to an individual’s peer group by determining any deviance from the mean and ranking the severity of that deviance. Consideration must be given to the patient’s baseline normal and whether that deviated from peers. Evaluation of how deficits impact function to determine whether the deficits lead to impairment for the individual is also essential. Finally, it is a healthy fear, or respect, for the impact of labels that should provide a cautionary guide in the analysis and interpretation stages of diagnosis, particularly as it relates to cognitive-linguistic deficits and disorders.
There has been increasing interest in and focus on evidence-based practice (EBP) in the field of Speech-Language Pathology (SLP) over recent years. EBP is a diagnostic and treatment process in which the clinician uses the best evidence available in conjunction with clinical expertise and the patient’s values to decide on the options that suit the patient best (2). EBP guidelines have been developed by the Academy of Neurologic Communication Disorders and Sciences (ANCDS) in collaboration with the American Speech Language Hearing Association and the US Department of Veterans Affairs. There has been criticism within the scientific process that few, if any, high-powered, randomized, controlled trials support the efficacy of speech therapy. Some argue that a randomized controlled trial does not lend itself well to the unique and individual variances that comprise each patient’s deficits within the clinical environment, particularly a heterogeneous population such as those with acquired brain injury. While the research and debate continue, there are fundamental methods, approaches, and techniques supported in the literature.
The process of evaluation and diagnosis begins with obtaining a thorough review of the patient’s history and physical information and a consult with the patient’s family and/or caregivers. If the client is an inpatient in the hospital, the SLP will communicate with the patient’s nurse to determine whether the patient is able to proceed with an evaluation.
Most often in the medical setting, the first and foremost reason to consult a SLP is to determine a patient’s ability to engage in safe oral intake; the risk for aspiration with oral intake; the ability to maintain nutrition and hydration via safe oral intake; the need for an alternate source to provide nutrition, hydration, and medication; and a prognosis of whether that required alternate source will be temporary or long term.
THE ORAL MOTOR EXAMINATION
The oral motor examination (OME) is an assessment of structure and function. The SLP will assess oral structure, mucosa, and cranial nerve function because they impact speech and swallowing and because they may signal neuropathology. Respiration, resonance, and articulation will be assessed at rest, during structured tasks, and dynamically in open context conversation. First, the SLP will assess facial symmetry both at rest and upon movement. Next, labial closure, rounding, and retraction will be tested. The tongue will be examined for lingual extension, and any deviation or fasciculations are noted; the tongue will also be examined for lateralization, atrophy, and strength against applied pressure. Speech alternating motion rates (AMRs) and sequential motion rates (SMRs) will also be evaluated. The hard and soft palates will be examined, noting any deformity and any deviation from complete, full, and strong retraction upon phonation. Vocal quality will be perceptually rated for vocal frequency, intensity, quality, and resonance (Table 10-1). Particular attention will be paid to the coordination of the articulatory, resonatory, and respiratory systems as they relate to speech, swallowing, and communicative ability.
Table 10-1.Sustained Phonation Maximum in Seconds for the Vowel /ah/
Median
Minimum
Maximum
Young males
28.5 (8.4)
22.6 (5.5)
34.6 (11.4)
Young females
22.7 (5.7)
15.2 (4.1)
26.5 (11.3)
Elderly males
13.8 (6.3)
13.0 (5.9)
18.1 (6.6)
Elderly females
14.4 (5.7)
10.0 (5.6)
15.4 (5.8)
AMRs and SMRs for Normal Adults
/puh/
6.3 (0.7)
5.0 (0.4)
7.1 (1.2)
/tuh/
6.2 (0.8)
4.8 (0.4)
7.1 (1.1)
/kuh/
5.8 (0.8)
4.4 (0.6)
6.4 (1.1)
/puh-tuh-kuh/
5.0 (0.7)
3.6 (0.3)
7.5 (1.3)
Derived from Duffy J. Motor Speech Disorders: Substrates, Differential Diagnosis, and Management. St. Louis: Mosby; 1995.
It is a complete and thorough OME that belies evaluation of dysarthria, oral or verbal apraxia, dysphagia, cognitive-communicative disorder, and aphasia. Any deviation from that which is considered within functional limits will be noted. Any deviation from that which is considered within normal limits will trigger further evaluation. For example, the OME of an individual who is edentulous and has no dentures is certainly not within “normal” limits; however, it may well be within “functional” limits. This individual may have been edentulous and eating a regular-consistency diet for many years with no difficulty. Another example may be an individual who underwent partial glossectomy secondary to cancer several years earlier, who has been eating a regular-consistency diet without difficulty. The key piece of information is whether the deviance from “normal” impacts safe and efficient oral intake and efficient and effective speech or communication.
ACQUIRED NEUROMUSCULAR SPEECH DISORDERS
Neuromuscular speech disorders include dysarthria and apraxia, two distinctly different disorders. Dysarthria refers to a speech disorder that results from a disturbance in muscular control over the speech mechanism due to damage of the central or peripheral nervous system, resulting in paralysis, weakness, or incoordination of the speech mechanism and leading to difficulty with oral communication (7). Dysarthria, in its most severe form, is characterized by anarthria (failure of structures to articulate).
The terms oral apraxia and verbal apraxia refer to a disorder of motor sequencing that is present in the absence of neuromuscular weakness. Severe oral and verbal apraxia is characterized by effortful articulatory groping to produce speech sounds; however, in its mild form, it may merely present as phonemic substitutions during open context conversation.
DYSARTHRIA ASSESSMENT
The diagnosis of dysarthria is based upon complete assessment of five characteristics: respiration, phonation, resonance, articulation, and prosody (Table 10-2). Standardized articulation protocols are more commonly used with children to determine whether the child is exhibiting a disorder of articulation or phonologic processes. This is not the case in the adult population. The Frenchay Dysarthria Assessment (11) is one commonly used protocol in the adult population. The Assessment of Intelligibility of Dysarthric Speech (AIDS) (29) is another.
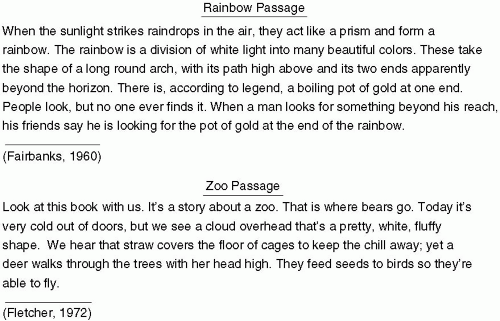
While there are a few standardized articulation protocols that may be used with adults, they are infrequently used in deference to a “speech sample” that is both tape recorded and transcribed and possibly videotaped in order to provide the patient with visual feedback of his or her own communication skills. As mentioned earlier, the combination of speech AMRs and SMRs and speech intelligibility for verbal production of basic needs/wants words, phrases, sentences, and paragraph levels are assessed. The most commonly used paragraphs are presented in Figure 10-1. Both paragraphs contain a fair sampling of all phonemes and phoneme combinations in the English language. In addition to having the patient read these passages, speech intelligibility is perceptually rated in open context conversation. Some individuals may not be able to see or read; therefore, accommodating the individual’s abilities and needs is essential in order to determine the patient’s baseline level and current status and assess for confirmatory signs.
Table 10-2.Differentiating the Dysarthrias
Lower Motor Neuron (LMN)
Upper Motor Neuron (UMN)
Unilateral Upper Motor Neuron (UUMN)
Hypokinetic
Hyperkinetic
Ataxic
Articulation
Imprecise; weak and floppy
Imprecise consonants
Imprecise; weakness on one side only—contralateral to lesion
Reduced lingual phoneme strength; increased rate
Involuntary movement; inconsistent overshooting for target consonant articulation
Inconsistent; imprecise consonants; excess and unequal stress; distorted vowels
Respiration
Breathy
Grunts at end of phrase
May be reduced capacity; may see clavicular breathing
Reduced capacity; increased rate; latency to begin exhalation
Myoclonic displacement of abdominal wall
Inconsistent
Phonation
Hypernasal
Strain-strangle; bulbar cry (sounds like a motor winding down)
Harsh
Hypophonic; monopitch; monoloud
Abnormal vowel prolongation
Pitch variation; intensity or loudness variation
Prosody
Short phrases
Slow; excess and equal stress
Slow
Rushes of short, blurred phrases
Variable rate; inappropriate silences
Staccato; inconsistent excess stress
Overall
Weakness; labial or lingual fasciculations are hallmark
Spasticity; strainstrangle vocal quality; bulbar cry is hallmark
Unilateral weakness; most amenable to voluntary control; thicktongued sounding
Masked facies; festinating gait; rigidity; hypophonic, monopitch, monoloud vocal quality with rushes of blurred, short phrases
Involuntary movements
Discoordination; (to the untrained ear, sounds as if drunk)
This is not intended to be a comprehensive list and does not include the various mixed dysarthrias.
DYSARTHRIA TYPES AND HALLMARK SIGNS
There are seven types of dysarthria that are dependent upon the location of the lesion (8). These are as follows:
Flaccid dysarthria is caused by a lesion in the lower motor neuron or final common pathway, resulting in weakness, paresis, paralysis, hypotonia, and atrophy. The presence of fasciculations is a confirmatory sign.
Figure 10-1. Phonemically balanced passages commonly used for speech sampling. (c) 2000 Douglas N. Honorof, Jill McCullough & Barbara Somerville. All rights reserved.
Unilateral upper motor neuron dysarthria is caused by a unilateral lesion located in the upper motor neuron. Speech intelligibility is impacted by location of weakness and compounded by discoordination. Speech will sound slurred, slow, and thick. Oral dysphagia is frequently a concomitant problem.
In spastic dysarthria, the lesion occurs in the upper motor neuron bilaterally and results in spastic, tight muscles. All five speech characteristics are affected. Often, short phrases are produced in a low monopitch. Resonance is hypernasal. A strain-strangled vocal cry or pseudobulbar cry is frequently seen. Hallmark signs include spasticity; weak, slow, reduced range of motion; degenerative conditions; slow and effortful articulation; appear to be speaking against resistance; fatigue; hypernasality; dysphagia; drooling; and emotional lability.
Ataxic dysarthria is typically noted when there is a cerebellar or brainstem lesion. Coordination and integration are affected. To the untrained ear, this speech disorder sounds much like “drunken speech.” Excessive loudness and unequal stress are features.
Hypokinetic dysarthria typically results from a lesion in the basal ganglia. Reduced range and amplitude of movement are exhibited. Speech articulation sounds are blurred, and voice is quiet. Patients typically benefit from use of prosodic cues such as a metronome and compensatory strategies that enable improved vocal intensity.
Hyperkinetic dysarthria also occurs in a basal ganglia lesion. Excessive, uncontrollable movement, involuntary hyperkinesias, and chorea are exhibited. Vocal quality is typically hypernasal, harsh, and loud in intensity. Speech articulation is characterized by inconsistent articulatory breakdown; there is no pattern. Dyskinesias are further broken down into nine types: hyperkinesia, myoclonus, tic, chorea, ballism, athetosis, dystonia, spasm, and tremor. Hyperkinetic dysarthria is not amenable to a specific dysarthria treatment unless the underlying movement disorder is medicated. Speech therapy services are beneficial to individuals and their family or caregivers initially and for a brief duration to provide education and counseling.
Mixed dysarthria lesions are, as the name implies, mixed or diffuse. This can be seen in traumatic brain injury (TBI), closed head injury (CHI), multiple sclerosis (MS), and amyotrophic lateral sclerosis (ALS). Therapy techniques are highly individualized and based upon which component contributes most to unintelligibility.
In anarthria, the lesions are typically in the cortex and cerebellum. If a patient’s mutism is related to a single lesion, it is likely brainstem. Patients are often speechless due to loss of neuromuscular control over the speech mechanism.
Figure 10-2. Flowchart for differentiating dysarthria from apraxia.
APRAXIA ASSESSMENT
Apraxia is an impairment in motor programming and is not due to weakness or paralysis of structures. Traditional characteristics include phonemic errors, perseverative and anticipatory misarticulations, and inconsistent articulatory approximations. Errors vary with increased complexity. For example, an individual may have little difficulty producing automatic speech phrases or overlearned passages or songs but increased difficulty for novel verbal productions. The patient will usually exhibit awareness of misarticulations and a great deal of frustration. Because of this frustration, the focus of therapy is initially generally placed on getting the message out and later on fine tuning the use of compensatory strategies such as slow rate, even stress, and even spacing between words.
APRAXIA VERSUS DYSARTHRIA
When determining whether a person has apraxia or dysarthria, the first characteristic to which attention must be paid is the patient’s struggle or “articulatory groping” as speech is attempted. The SLP will have previously noted on the OME whether the patient demonstrated “articulatory groping” when attempting various oral postures upon command (e.g., grimacing when asked to open the mouth, lingual extension when asked to puff up the cheeks, squinting when asked to demonstrate pursing the lips and blowing). If no asymmetry or weakness is demonstrated on OME and no effortful struggle is apparent when performing volitional oral postures, verbal apraxia may be present. Phonemic substitutions are quite commonly exhibited in verbal apraxia, even if no effortful articulatory groping is demonstrated when volitionally producing various oral postures for the OME. For example, an individual may say “The clog jumped off the cliff” or “The dog jumped off the diff” when asked to read “The dog jumped off the cliff.” Individuals with verbal apraxia will likely exhibit difficulty repeating words of increasing length (e.g., back, backhand, backhanded; increase, increasing, increasingly). Difficulty will be exhibited for multisyllabic words. They will often report, “I know the word, I just can’t say it.” They may well exhibit no difficulty when reading a printed paragraph aloud and then an inordinate amount of difficulty during conversation.
Differentiating between apraxia and dysarthria is fundamental in order to initiate the correct treatment approach. Excessive repetition and practice are essential treatment techniques for verbal apraxia; whereas, they would be ineffective and inappropriate for some types of dysarthria (e.g., mixed flaccid-spastic dysarthria seen in ALS or flaccid dysarthria seen with myasthenia gravis). Figure 10-2 illustrates basic considerations for diagnostic differentiation of dysarthria and apraxia.
Only gold members can continue reading. Log In or Register to continue