Age-Related Changes in Pharmacokinetics, Drug Interactions, and Adverse Effects
Age-Related Changes in Pharmacokinetics, Drug Interactions, and Adverse Effects
James C. Cloyd
Jeannine M. Conway
Older adults (65 years of age or older) comprise 13% of the population and account for 35% of all prescription expenditures ($12.7 to $14.3 billion in 1991), and more than 69% of the elderly have more than one chronic medical condition (53,116). Community-dwelling older adults are reported to take, on average, 3.1 to 7.9 prescription and nonprescription medications, whereas nursing home residents have an average of 8.8 medication orders, with 32% of residents taking more than nine medications (23,119). Adults older than 65 are at double the risk for adverse drug reactions (ADRs) compared with younger adults, and they are more than seven times more likely to be hospitalized (10). Neuropsychiatric medications are among the most common causes of ADRs (10,65,111). Age alone does not appear to be a risk factor for ADRs, but older adults are at greater risk because they take a larger number of medications and have a greater number of medical problems (12,49,51). Alterations in pharmacokinetics and pharmacodynamics can also increase the ADR susceptibility in older adults, but no well-controlled studies have evaluated their influence on ADRs (51). Problems associated with drug therapy in the elderly will likely become even more pronounced with the rapid rise in the population of the oldest old (≥85 years of age). Individuals ≥85 years old are projected to increase in number by 2050 to 5% of the U.S. population (124). Age-related changes in parameters necessitate a different approach to drug therapy in the elderly and place the older patient at greater risk for serious drug interactions and adverse events compared with younger adults. An understanding of the effects of advancing age on drug disposition and response and the mechanisms by which interactions occur permits the clinician to rationally prescribe and more effectively manage neuropsychiatric drug therapy in the older patient.
Table 4-1.Age-Related Changes in Physiology
Absorption
Gastrointestinal blood flow
↓
Absorption
↔
Gastric pH
↓
Gastric emptying
↓
Intestinal motility
↓
Distribution
Lean body mass
↓
Body fat
↑
Plasma albumin
↓↔
Metabolism
Liver mass
↓
Hepatic blood flow
↓
Excretion
Kidney mass
↓
Renal blood flow
↓
Glomerular filtration
↓
Filtration fraction
↓
AGE-RELATED CHANGES IN PHYSIOLOGY: EFFECT ON PHARMACODYNAMICS AND PHARMACOKINETICS
The marked alterations in physiology that occur with advancing age affect both the pharmacokinetics and pharmacodynamics of drugs used to treat neuropsychiatric disorders. Changes in pharmacokinetics result in either higher or lower drug concentrations, depending on the variable contributions of absorption and elimination. Response, either beneficial or adverse, can be exaggerated or diminished even when the plasma drug concentration is unchanged. Physiologic changes affecting all aspects of drug disposition—absorption, distribution, metabolism, and elimination—occur as a person ages (Table 4-1). Aging also alters the number and function of central nervous system (CNS) receptors that determine the nature and intensity of response to drugs (103). Many diseases common to the elderly alter pharmacokinetics, pharmacodynamics, or both.
ABSORPTION
Drug absorption is influenced by several anatomic and physiologic factors, including gastric emptying, gastric and intestinal pH, quantity and quality of bile secretions, intestinal motility, condition and number of absorptive cells, enterocyte efflux, metabolizing enzymes, and intestinal blood flow (5,135). Absorption is also dependent on a drug’s physical and chemical properties, such as release from the dosage form, dissolution, and lipophilicity (29).
No significant age-related change appears to exist in the anatomic features of the small intestine (73). Contrary to conventional wisdom, only a small percentage of the elderly (>70 years) have lost the ability to secrete acid due to chronic atrophic gastritis (54, 55). Pharmacotherapy with proton pump inhibitors results in an artificial achlorhydria, which may impact drug absorption. Gastric pH is important for drugs, including iron salts, ketoconazole, and ampicillin, that require an acidic pH for absorption (57). Gastric emptying can be decreased by half in 25% of the elderly greater than 70 years of age (27). Reduced motility will result in a longer residual time for medications and can affect absorption, depending on a drug’s chemical properties. If a medication is rapidly absorbed because it readily dissolves and easily diffuses across luminal membranes into systemic circulation, changes in motility are unlikely to affect absorption. Drugs that are slowly absorbed because of poor aqueous solubility or decreased diffusion rate will exhibit increased bioavailability because of a longer resident time in the absorptive segment of the small intestine (29). Blood flow to the gastrointestinal tract is reduced with age; theoretically, this could result in decreased absorption of some drugs, but there is insufficient evidence to determine whether this is clinically important (5).
Until recently, it was assumed that the mechanism for drug absorption across the intestinal mucosa was passive diffusion. Active influx and efflux transport enzymes are now known to play a role in both the rate and extent of absorption. Gabapentin bioavailability is primarily mediated by an L-amino acid transport system that becomes saturated at clinically relevant doses (118). P-glycoprotein (P-gp), an efflux transporter located in intestinal enterocytes, pumps medications out of the cell and into the intestinal lumen, thereby decreasing drug absorption (129). P-gp is expressed in many tissues, including the adrenal cortex, brush border of the proximal renal tubule epithelium, pancreatic ductules, luminal surface of biliary hepatocytes, immunomodulation cells, blood-brain barrier, and the mucosa of the small and large intestines (69). P-gp is responsible for excreting 16% of an intravenous dose of digoxin into the gut lumen in mice, whereas only 2% of the dose was excreted in a P-gp knockout mouse (77). Certain drugs can either induce or inhibit P-gp, resulting in a decrease or increase in the bioavailability of the affected medication (34). Finally, drug absorption is affected by the presence of drug-metabolizing enzymes in the gastrointestinal mucosa. Cytochrome P450 (CYP) enzymes, which are located in intestinal enterocytes, can have a substantial impact on absorption (70). Midazolam, a CYP3A4 substrate, has a bioavailability of >90% following intramuscular administration but approximately 36% when given by mouth (96). The difference is largely attributable to metabolism in the gut wall. It is not known whether either the amount or function of P-gp or CYP enzymes in the gut changes with age.
Age-related changes in gastrointestinal physiology do not have a predictable effect on drug absorption. Most importantly, age-related changes in gastric function both within a patient and among patients may be highly variable. These unpredictable changes may alter the bioavailability of slowly absorbed drugs and should be considered when changes in response occur.
DISTRIBUTION
Drug distribution has two components: the extent to which the drug distributes throughout the body and the percentage bound to plasma proteins. Both are altered in old age. The distribution of a drug is partially dependent on its polarity. Highly polar compounds are hydrophilic and tend to distribute mainly into extracellular water. Lipophilic drugs tend to distribute mainly into tissue compartments, particularly muscle and fat. Age-related changes in body composition will alter volume of distribution (Vd). The percentage of body fat increases and lean body mass decreases with age (24,31,113). This shift in body composition may cause an increase in the Vd for lipophilic drugs and a decrease in the Vd for hydrophilic drugs.
Distribution volume is the key parameter in calculating loading doses, as is shown in the following equation: Loading dose = (Concentration desired—baseline concentration) * wt in kg * Vd ( L/kg).
Distribution volume is usually determined from studies in younger adults. The elderly may have an unexpected response to a medication because their Vd deviates from the average younger adult values, resulting in a subtherapeutic or toxic plasma drug concentration.
Advancing age affects the extent to which CNS drugs bind to plasma proteins. Medications may bind to albumin, alpha1-acid glycoprotein, globulins, and lipoproteins. Some drugs (e.g., zonisamide and topiramate) may also bind to erythrocytes (38,60,91). In the older adult, albumin, on average, declines slightly with age (11,44). Other conditions common in the elderly such as renal insufficiency, rheumatoid arthritis, and malnutrition also reduce albumin concentrations (44,128). In contrast, alpha1-acid glycoprotein, which binds alkaline drugs, increases with age, and further elevations can occur from conditions such as stroke, heart failure, infection, trauma, myocardial infarction, arthritis, surgery, and chronic obstructive pulmonary disease (128).
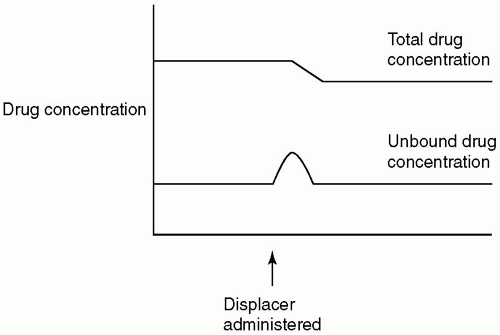
Figure 4-1. Effect of changes in protein binding and clearance on total concentration and unbound concentrations.
Only drugs protein-bound by 80% or more are significantly affected by alterations in plasma proteins. Most disruptions in binding are clinically unimportant but can cause a misinterpretation of drug concentrations. As shown in Figure 4-1, a decrease in protein binding results in lower total, but not unbound, concentrations for low hepatic extraction drugs. This occurs because only unbound drug in plasma diffuses into the hepatocyte or renal cell, where it is either metabolized or excreted. At steady-state, the dose and the clearance of unbound drug determine the unbound concentration in plasma. Drug freed from protein-binding sites (e.g., because of decreased albumin) becomes available for elimination. Because neither daily dose nor unbound clearance changes, unbound drug concentrations remain the same. Alterations in plasma proteins can complicate interpretation of laboratory values of highly bound drugs such as phenytoin (PHT). PHT is normally 90% bound to albumin. At a total PHT concentration of 15 mg/mL, the unbound concentration is 1.5 mg/L. This relationship can change over time as an elderly patient experiences a decline in plasma albumin. In such a patient, binding can decline to 80%, resulting in a total concentration of 7.5 mg/L, whereas the unbound concentration remains at 1.5 mg/L. In this situation, an increase in dose is not indicated.
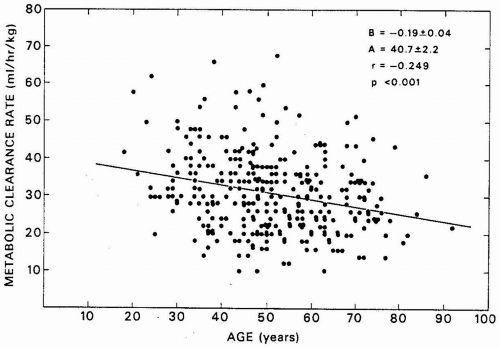
Figure 4-2. Effect of advancing age on antipyrine clearance. (From Vestal RE, Norris AH, Tobin JD, et al. Antipyrine metabolism in man: influence of age, alcohol, caffeine, and smoking. Clin Pharmacol Ther. 1975;18 (4):425-432.)
METABOLISM
The two most important age-related physiologic changes that occur in the liver are decreased mass and reduced blood flow (Fig. 4-2). Wynne et al. (134) examined changes in liver mass (as assessed by ultrasound) and liver blood flow (indocyanine green clearance) with respect to age in men. Sixty-five patients were divided into three groups (<40, 40 to 64, and >65 years), with 20 patients over the age of 65. A 21% decrease in liver volume (in relation to body weight) was observed in the elderly male population. A 28% reduction in liver blood flow was also observed. The impact of advancing age on drug metabolism has been primarily studied in healthy, ambulatory subjects aged 65 to 75 years. No information is found regarding hepatic changes in the oldest old (≥85 years) or in frail older patients. Both groups are likely to have diminished drug-metabolizing capacity relative to younger, healthier elderly adults.
Hepatic metabolism is divided into two phases. Phase I consists of oxidative, reduction, and hydroxylation reactions. The CYP family of enzymes generally catalyzes the oxidative reactions. Phase II reactions are conjugation reactions involving glucuronic acid or sulfates in which conjugated product is made more polar, allowing it to be excreted into the urine or bile. Conjugation reactions can involve either the drug (primary conjugation) or the metabolite of a phase I reaction (132).
The CYP system consists of a family of closely related enzymes known as isoenzymes, each of which catalyzes the metabolism of a unique set of substrates. Table 4-2 lists the major isoenzymes that catalyze the metabolism of numerous neurologic drugs. Available evidence indicates that CYP metabolizing activity declines approximately 1% a year beginning at age 40, although substantial intrapatient variability is seen (115). Antipyrine metabolism is associated with CYP metabolism, and clearance of antipyrine declines with age, as shown in Figure 4-2.
Many CNS drugs that undergo either primary or secondary metabolism via conjugation reactions with glucuronic acid are mediated by uridine glucuronyl transferases (UGT) (4,125). As with the CYP system, UGTs are composed of isoenzymes with specific drug substrates (99). The effect of age on glucuronidation is less well understood than the CYP system. Greenblatt et al. (45,46) and Divoll et al. (21) studied the pharmacokinetics of several benzodiazepines (oxazepam, temazepam, and lorazepam) that undergo extensive glucuronidation in elderly patients, most of whom ranged in age from 65 to 75 years. Drug clearance was similar in elderly and younger subjects. The studies gave rise to the view that glucuronidation activity is spared in the elderly.
EXCRETION
Many drugs and their metabolites are eliminated completely or partly by the kidney. Age-related changes in renal function are well established (71,82,93,109). Anatomic changes result in decreased kidney size, decreased renal blood flow, a loss of glomeruli, and renal tubular changes (82,93). Functional changes include a decrease in glomerular filtration, decreased creatinine clearance, and increased serum creatinine concentrations (108). Renal function decreases begin at age 40, resulting in a 40% decline in renal function by age 70 as compared with age 30 (72).
Reductions in renal function will result in a decrease in the clearance of drugs eliminated by the kidney. Serum creatinine is not a reliable marker of renal function in the elderly because creatinine is a byproduct of muscle and, as individuals age, lean body mass and serum creatinine decline (86). For example, a serum creatinine level (SCr) of 1.0 mg/dL, which is within the normal range, does not accurately estimate the creatinine clearance in a 41-kg woman who is 80 years of age. An estimated creatinine clearance (ClCr) adjusted for age, gender, and weight (when a patient is within 30% of his or her ideal body weight) provides a better indicator of renal function in the elderly (17). In most patients, an estimate of creatinine clearance can be used to adjust dosage. One such method is the Cockcroft-Gault equation:
Using this equation, a woman 80 years of age would have an estimated creatinine clearance of 25 mL/min, necessitating a substantial change in dose for drugs such as gabapentin, which is virtually 100% renally eliminated. In contrast a 65-kg woman who is 30 years of age with a serum creatinine of 1.0 mg/dL would have an estimated creatinine clearance of 84 mL/min. Although an improvement over the use of an unadjusted SCr, the Cockcroft-Gault equation has its own limitations. In a healthy elderly patient, it may underpredict renal function, resulting in subtherapeutic dosing, and if the patient is frail, it may overpredict renal function, resulting in unexpected toxicity (30). The available evidence supports the conclusion that drug elimination via renal excretion or metabolism by either phase I or phase II declines with advancing age, although there is considerable variability. As a general rule, elderly patients should initiate therapy at a dose 30% to 50% less than younger adults, and dosing intervals can be extended as the elimination half-life is prolonged.
PHARMACODYNAMICS
Pharmacodynamics is the major source of variation in drug response (67). Age-related changes in pharmacodynamics are drug specific and can result in greater or diminished responses (16). Studies indicate that the elderly are more sensitive to CNS depressants than younger adults. Following administration of the same dose of diazepam, elderly patients experienced more pronounced sedative effects, although unbound serum concentrations were comparable to those observed in younger adults (18). Older adults also exhibited exaggerated sedative effects after administration of midazolam, although the dose was reduced for the elderly study group and both groups had similar plasma concentrations (98). Little information is found about altered pharmacodynamics of other CNS drugs with age. It is reasonable to conclude that CNS depressants are likely to produce a greater effect in the elderly than in younger adults, even when doses are adjusted.
Table 4-2.CYP Enzymes Responsible for Neurologic Drug Metabolism and Their Induction and Inhibition
1A2
2C9
2C19
2D6
3A4
Substrates
Caffeine
Fluoxetine
Citalopram
Amitriptyline
Alprazolam
Carbamazepine
Phenytoin
Clomipramine
Desipramine
Carbamazepine
Clozapine
Valproic Acid
Diazepam
Donepezil
Citalopram
Fluvoxamine
Felbamate
Duloxetine
Clonazepam
Mirtazapine (minor)
Imipramine
Fluoxetine (minor)
Clozapine
Olanzapine
Phenytoin (minor)
Fluvoxamine
Donepezil
Ropinirole
Sertraline (minor)
Galantamine
Eszopiclone
Tacrine
Haloperidol
Galantamine
Imipramine
Haloperidol
Mirtazapine (minor)
Midazolam
Nortriptyline
Mirtazapine
Paroxetine
Nefazodone
Perphenazine
Ropinirole (minor)
Risperidone
Sertraline (major)
Sertraline
Tiagabine
Thioridazine
Triazolam
Venlafaxine
Zaleplon
Ziprasidone
Zolipidem
Zonisamide
Inducers
Omeprazole
Carbamazepine
Carbamazepine
Carbamazepine
Tobacco
Phenobarbital
Phenytoin
Oxcarbazepine
Rifampin
Rifampin
Phenobarbital
Phenytoin
Rifampin
St. John’s Wort
Inhibitors
Cimetidine
Fluconazole
Cimetidine
Bupropion
Clarithromycin
Ciprofloxacin
Fluoxetine
Felbamate
Cimetidine
Diltiazem
Fluvoxamine (moderate)
Fluvoxamine
Fluconazole
Clomipramine
Erythromycin
Fluoxetine
Duloxetine (moderate)
Fluconazole
Fluvoxamine
Fluoxetine
Fluoxetine (moderate)
Omeprazole
Paroxetine
Fluvoxamine (moderate)
Oxcarbazepine
Grapefruit juice substances
Sertraline (moderate)
Itraconazole
Topiramate
Ketoconazole
Nefazodone
Note: This table is not all inclusive. The authors recommend that all practitioners use drug interaction references or databases to check for potential interactions when prescribing medications.
Only gold members can continue reading. Log In or Register to continue