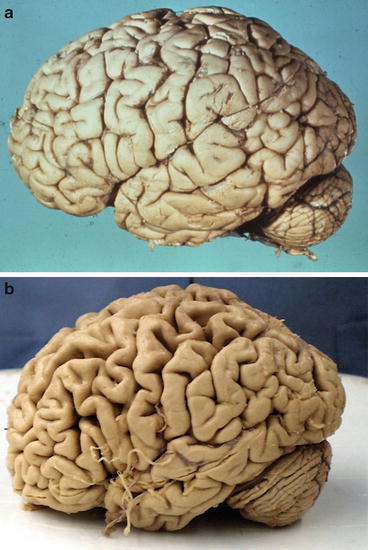
Fig. 2.1
Normal brain. (a) The lobes gyri and major sulci labeled in the frontal, parietal, occipital, and temporal gyri, and the motor strip identified on the lateral surface of the brain. (b) Medial surface with the corpus callosum, fornix, and gyri and cingulate sulci labeled and the gyri and sulci in the frontal, parietal, occipital and temporal lobe labeled. (c) Frontal and parietal operculum removed to reveal insular cortex and auditory cortex of temporal lobe (transverse temporal gyri). (From Jacobson and Marcus [17])
Group One- CVA/Strokes
Worldwide, cardiac disease and stroke are the most common causes of death in the middle and upper income countries while in the lower income countries respiratory infections is the most common cause, followed by diarrheal disease, HIV AIDS and then ischemic heart disease, as the fourth most common, followed by malaria and then stroke [5].
In the USA as noted in the most recent data from the CDC in 2011, cardiac disease is the most common cause of death (597,689) with cancer as second (574,743), chronic lower respiratory diseases third (138,080) and CVA/stroke the fourth most common cause of death (129,476). Alzheimer’s Disease is the 6th most common cause of death (83,494). Strokes also are the most common cause of degeneration in the brain and untreated hypertension in many cases is the root cause and can lead to strokes, ministrokes/TIAs, mild cognitive dysfunction and dementia. The following cases illustrate these points.
A 62 year old, Left-handed, untreated male with hypertension had an infarct in the territory of the middle cerebral artery on the left after carotid clamping for removal of plaque in the left common carotid. The patient progressed from a weakness of the right hand to complete right hemiparesis with right central facial weakness and a mixed aphasia. There was a subsequent recovery in the right lower extremity. Figure 2.2 is the post mortem examination of the brain of Patient One showing an infarct in the right operculum of the precentral gyrus and insula.
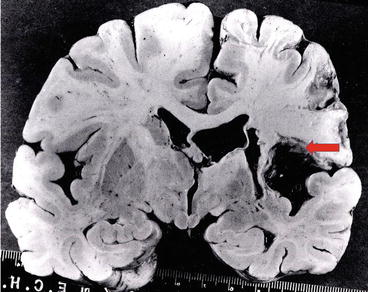
Fig. 2.2
CVA. This is a post mortem examination of the brain of Case One with a CVA showing an infarct in the left operculum of the precentral gyrus and insula (From Jacobson and Marcus [17])
Figure 2.3a is an MRI which shows the appearance of a normal patient at the level of the frontal operculum, while Fig. 2.3b is an MRI which shows an infarct in the cortical territory of the left superior branch of the middle cerebral artery in the frontal lobe with similar neurological findings to Case One.
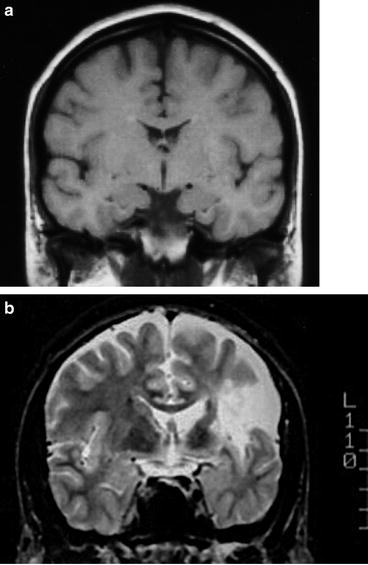
Fig. 2.3
CVA. (a) is an MRI which shows the appearance of a normal patient at the level of the frontal operculum, while (b) is an MRI which shows an infarct in the cortical territory of the left superior branch of the middle cerebral artery in the frontal lobe with similar neurological findings to Case One (From Jacobson and Marcus [17])
Figure 2.4 is a micrograph which demonstrates a lesion in the right medullary pyramid several years after a lesion in the medial most portion of the left motor strip with resultant atrophy of the corticospinal pathway and resultant upper motor deficit with increased reflexes, weakness of movements and some disuse atrophy of the right lower leg.
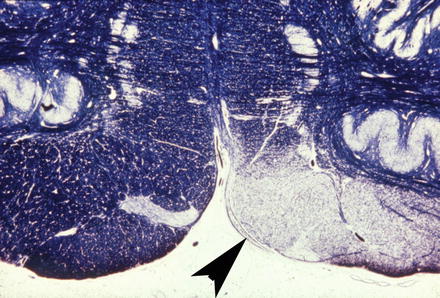
Fig. 2.4
CVA. This micrograph demonstrates a lesion in the right medullary pyramid several years after a lesion in the medial most portion of the left motor strip (controls the contralateral foot). This patient demonstrated atrophy of the corticospinal pathway and clinically demonstrated an upper motor deficit with increased reflexes, weakness of movements and some disuse atrophy of the right lower leg (From Jacobson and Marcus [17])
Although cardiac disease is still the most common causes of death in middle and upper income countries, there have been improvements due to better nutritional choices, exercise, stopping smoking, reducing salt intake and taking of medicine which will reduce the blood pressure. In lower income countries as shown in a recent article in Neurology [18] there is a critical need to alleviate the effects of hypertension, by encouraging life style changes, and reducing salt intake and when necessary treating patients with the inexpensive anti hypertensives (thiazides). The National Institute of Neurological Disease and Stroke of the National Institute of Health is dedicated to the eradication and treatment of stroke in the USA and the world www.ninds.nih.
Group Two: Communicable Diseases, Malaria and HIV/AIDS
Case Two: Cerebral Malaria, Case developed by Dr. Erisa Mwaka Sabakaki, Fig. 2.5
A 32-year-old man presented with a history of fever, chills and weakness for 2 weeks along with generalized tonic-clonic seizures, occurring 2–3 times per day, for 5 days. He also had a history of loss of consciousness 2–3 times a day, each episode lasting for 2–3 min. He complained of loss of power in the right upper limb for 4 days. He had had 4–5 episodes of severe vomiting during the duration of the illness. CNS examination revealed that he was conscious and oriented. There was no neck rigidity. Power in the right upper limb was 4/5. His sensory and motor systems were normal; there was no cranial nerve deficit. The other systemic examinations were normal. Biochemical and hematological investigations were normal. Peripheral smear for malarial parasite was positive and the patient was started on antimalarial drugs. CT of the brain revealed an irregular lesion, mixed hyper- and hypodense areas in the left high posterior frontoparietal region and the evidence of a subdural and subarachnoid hematoma in left frontoparietal region with surrounding hypodensity. Two days later, the patient complained of pain and swelling in the left lower limb. Venous Doppler of the limb showed deep vein thrombosis. The patient was treated aggressively with antithrombotics, antibiotics, antipyretics and anti-inflammatory drugs along with antacids. The patient completed the course of antimalarial drugs. He improved clinically. Follow-up CT scan of the brain done 1 month later showed a resolving infarct in the left frontoparietal region.
Figure 2.5 is a CT of a patient demonstrating a large subdural (arrow) external to the frontal lobe with a shift of the midline and the compression of the lateral ventricles on the right and enlargement of the ventricles on the left due to the presence of the f. plasmodium parasites in the subdural space and also in the adjacent parenchyma of the infected brain. It has been noted that the parasites sequester in cerebral capillaries and also produce additional intra- and perivascular pathology with retinopathy being very common [19, 20]. Malaria is caused by a bite from an infected female anopheles mosquito carrying the protozoan parasites of falciparum plasmodium. It affects over 650,000,000 people infected each year and causes 10 % of the deaths in the lower income countries including Uganda (1–3,000,000/year; [5]). It also is a major cause of poverty and hinders economic growth. There has been some progress in protecting children by providing mosquito nets but more help is needed, and there has been some progress in developing a vaccine. We have developed a video (Cerebral malaria, www.braindementia.org) from a case of Cerebral Malaria which demonstrates cortical atrophy, a subdural haematoma and dilation of the ventricles, a common finding in Malaria (www.cdc.gov/malaria).
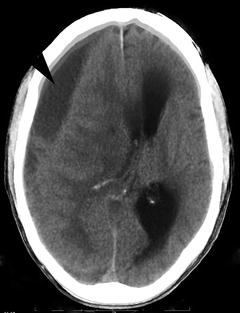
Fig. 2.5
Malaria. This CT is from a patient with a subdural hematoma and a displacement of the midline and compression of the lateral ventricles on cerebral malaria (From Kampala Imaging Center, courtesy of Dr. Rosemary Byanyima)
Case Three: HIV/AIDS (Fig. 2.6)
A 38 year old female presented with left sided hemiplegia and weakness on the right side and dementia (Fig. 2.6). She has recently started on antiretroviral therapy with some success. Her CD4 was 455 cells/mm. The CT images shows lesions on the right (1) and left (3) rostral internal capsule and a lesion in the insular cortex on the right (3) all of which were consistent with HIV infection in the brain [21, 22]. These pathological findings are consistent with other studies that have shown similar infarcts due to HIV-associated toxoplasmosis, tuberculosis and cryptococcosis whose presence were not tested for in this patient. Our findings of dementia in this patient were supported by the brain atrophy which was noted with the widening of the sulci in the young woman. Poor care of patients with limitations in extensive investigations is not uncommon in LIMC settings. The cause of HIV is well documented. There is still no cure for HIV. There is antiretroviral medication which slows the progression from HIV to AIDS, and it can keep many people healthy for many years. However, these medicines are not widely available in poor countries. There are many groups working on developing a vaccine for HIV/AIDS and they have not yet succeeded, but there is a sense of optimism that there will be a vaccine 1 day.

Fig. 2.6
HIV. This CT image of the brain is from Case Three. A 38 year old female presented with left sided hemiplegia and weakness on the right side and dementia. The CT images shows infarcts on the right (1) and left (2) in the rostral internal capsule and an infarct in the insula cortex on the right (3) due to the HIV infection. There is also significant evidence of brain atrophy with the widening of the sulci in this young woman (From the Kampala Imaging Center, courtesy of Dr. Rosemary Byanyima)
Uganda is often held up as a model for Africa in the fight against HIV and AIDS [23, 24]. In Africa in most cases, HIV is spread heterosexually. Other causes include mother-to-child transmission, transfusion with infected blood or sharing needles in intravenous drug use. There are an estimated 1.2 million people living with HIV in Uganda, which includes 150,000 children. Strong government leadership, broad-based partnerships and effective and extensive public education campaigns using bill boards, newspapers, the radio, TV and internet are all contributing to a decline in the number of people living with HIV and AIDS. Uganda’s success story must not detract from the consequences that AIDS continues to have across the country. An estimated 64,000 people died from AIDS in 2009 and over one million children have been orphaned by this devastating epidemic. The CDC has a very active surveillance and information upon the treatment of HIV (http://www.cdc.gov/hiv/topics/surveillance/) as does the WHO (http://www.who.int/hiv/en.)
Group Three (NCD) Neurodegenerative Diseases
A 64 year old male over the last 4 years had been having problems at work including inappropriate behavior, dress and memory problems. His changes in appearance and behavioral abnormalities including threatening his wife led him to be institutionalized by his family which was a very difficult experience for his wife and children (case developed by Drs. E. M Marcus and Stanley Jacobson). In Fig. 2.7a we show the appearance of a control brain while in Fig. 2.7b we show a brain from a patient diagnosed with Alzheimer’s Disease showing major widening of the sulci throughout the brain due to the decrease in cortical gray matter/gyri which is the major pathology seen with this disease. In Fig. 2.8a we have included an MRI from a patient without AD at age 91 with a normal appearing hippocampus while in comparison we have included the MRI from a 71 year old male with severe AD. Figure 2.8b is from a 76 year old patient defined clinically as having AD and it shows severe atrophy of the hippocampus (from Marcus and Jacobson [25]). Please note that there is also atrophy in the hippocampus of the patients with AD enlargement of the ventricle due to the degeneration of the brain.
 A Case Report of Mania and Glioma
Environmental Toxins as Causes of Brain Degeneration in Sub-Saharan Africa
A Case of Alzheimer’s Dementia in Uganda
Vitamin Deficiencies and Neuropsychiatric Disorders in Sub-Saharan Africa
A Case Report of Mania and Glioma
Environmental Toxins as Causes of Brain Degeneration in Sub-Saharan Africa
A Case of Alzheimer’s Dementia in Uganda
Vitamin Deficiencies and Neuropsychiatric Disorders in Sub-Saharan Africa
 Caring for the Elderly with Dementia in Africa
Caring for the Elderly with Dementia in Africa
 Review of Reasons for Patients to Receive a CT of the Head and Neck Region in Uganda in 2011–2012
Review of Reasons for Patients to Receive a CT of the Head and Neck Region in Uganda in 2011–2012




Related posts:
A Case Report of Mania and Glioma
Environmental Toxins as Causes of Brain Degeneration in Sub-Saharan Africa
A Case of Alzheimer’s Dementia in Uganda
Vitamin Deficiencies and Neuropsychiatric Disorders in Sub-Saharan Africa
Caring for the Elderly with Dementia in Africa
Review of Reasons for Patients to Receive a CT of the Head and Neck Region in Uganda in 2011–2012
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
