15 Anatomy of the Orbit and Related Structures
Helder Tedeschi and Albert L. Rhoton, Jr.
 Introduction
Introduction
Endoscopy has inaugurated a new era in the treatment of lesions located at the skull base. The concept of minimally invasive surgery has been broadened by the use of the endoscope, and many of the so-called surgically inaccessible areas can now be safely reached with considerably lower morbidity. New techniques of reconstruction have also substantially lessened the surgical complications. Being in close proximity with the nose and the paranasal sinuses, the optic canal and the medial and inferior walls of the orbit can be surgically approached with the aid of the surgical endoscope.
This chapter thoroughly describes the microsurgical anatomy of the orbital contents, which is important to the various surgical approaches directed to the orbit.
 Anatomy of the Orbit
Anatomy of the Orbit
The orbit is a complexly organized group of neural, vascular, muscular, ligamentous, and osseous structures that opens onto the face and external world to collect and provide binocular visual information to the brain.
Nearly all of the bones forming the anterior and middle cranial base contribute to the formation of the orbit’s walls. The orbit communicates posteriorly with the anterior and middle cranial fossae and inferiorly with the pterygopalatine and infratemporal fossa. The nerves and vessels entering and exiting the orbit pass through the optic canal and superior orbital fissure, which are partially surrounded by an annular tendon, from which the recti muscles arise.
The fact that many of the neural and vascular structures entering the orbit pass through not only an osseous channel but also through the annular tendon creates an added complexity when considering approaches to the orbit, and especially those involving the orbital apex. The orbit can be approached surgically from anteriorly through the face and conjunctivae or through any of its walls and from intracranially. The most common neurosurgical approaches are directed through the superior and lateral walls to lesions located deep in the orbit, near the apex or involving the optic canal, superior orbital fissure, and adjacent areas.1–3 Endoscopic approaches are somewhat restricted to the structures of the orbit that are related to the paranasal sinuses, which include the optic canal and the medial and inferior walls of the orbit.
 Osseous Relationships
Osseous Relationships
The walls of the orbit are formed by seven bones: frontal, zygomatic, sphenoid, lacrimal, ethmoid, and palatine bones and the maxilla (Fig. 15.1). The upper border of the orbital opening is formed by the frontal bone, which is notched or is the site of one or several small foramina that transmit the supraorbital and supratrochlear nerves and vessels. The lateral border of the orbital opening is formed by the frontal process of the zygomatic bone, except for the upper part, which is formed by the zygomatic process of the frontal bone. The lower margin of the orbital opening is formed laterally by the zygomatic bone and medially by the maxilla. The upper part of the medial border is formed by the frontal bone, and the lower part is formed by the frontal process of the maxilla. The medial part of the upper border contains the frontal sinus. The anterior part of the orbital roof is formed by the orbital plate of the frontal bone, and the posterior part is formed by the lesser wing of the sphenoid bone, which also forms most of the sphenoid ridge (Figs. 15.1 and 15.2). The sphenoid and ethmoid bones are interposed between the orbital roofs. The ethmoid bone is the site of the cribriform plate and the upward-projecting crista galli to which the falx attaches. Anteriorly, the frontal bone splits into two laminae, which enclose the frontal sinuses. The lacrimal fossa, the depression in which the lacrimal gland rests, is located below the anterolateral part of the roof.
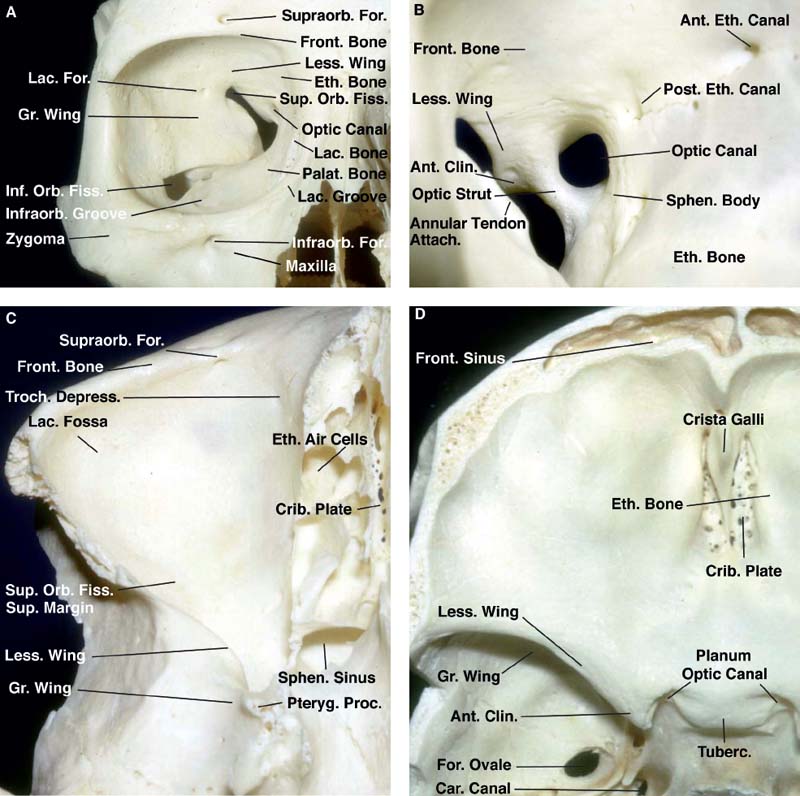
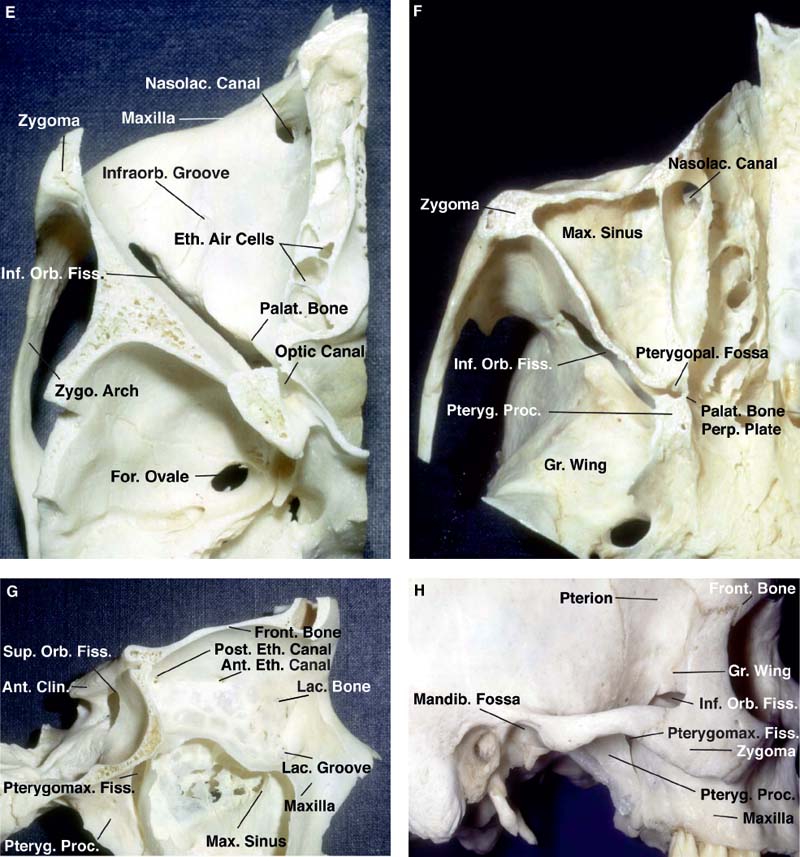
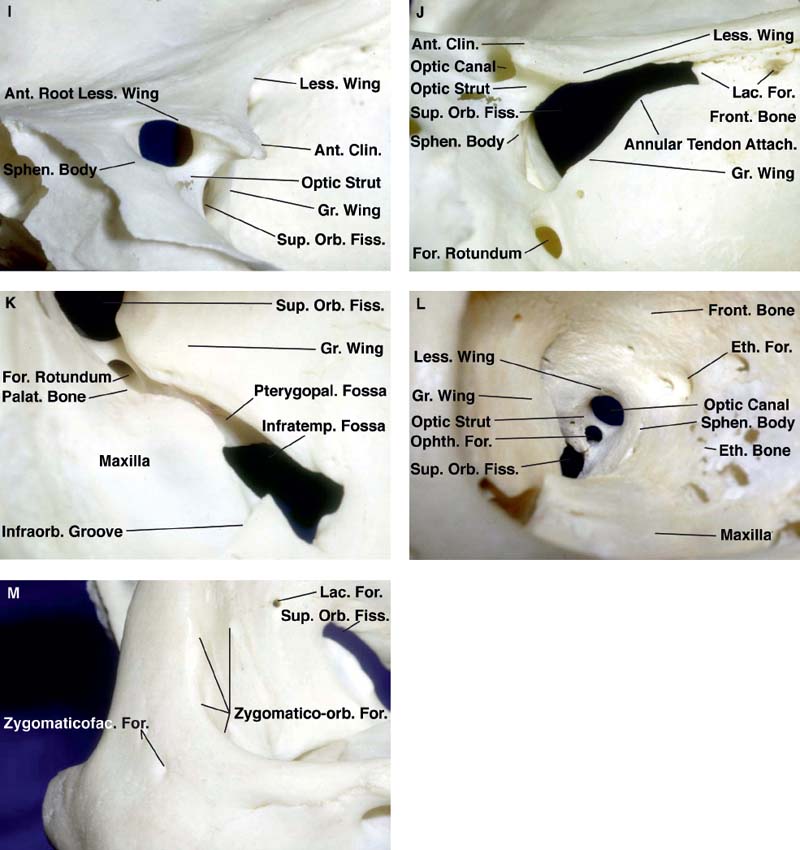
Fig. 15.1 Osseous relationships of the orbit. (A) Anterior view of the right orbit. (B) Anterior aspect of the right optic canal. (C) Roof of the right orbit viewed from below. (D) Superior aspect of the floor of the anterior cranial fossae that forms the roof of both orbits. (E) Floor of the right orbit viewed from above. (F) Inferior aspect of the roof of the maxillary sinus, which also forms the floor of the orbit. (G) Lateral view of the medial wall of the right orbit. (H) Lateral aspect of the lateral wall of the right orbit. (I) Intracranial aspect of the right optic canal. (J) Intracranial aspect of the right superior orbital fissure. (K) Orbital aspect of the right inferior orbital fissure. (L) Anterior aspect of the right optic canal and an anomalous ophthalmic foramen. (M) Anterolateral view of the right zygomaticofacial foramina. Ant.: anterior; Attach.: attachment; Car.: carotid; Clin.: clinoid; Crib.: cribriform; Depress.: depression; Eth.: ethmoid: ethmoidal; Fiss.: fissure; For.: foramen; Front.: frontal; Gr.: greater; Inf.: inferior; Infraorb.: infraorbital; Infratemp.: infratemporal; Lac.: lacrimal; Less.: lesser; Mandib.: mandibular; Max.: maxillary; Nasolac.: nasolacrimal; Ophth.: ophthalmic; Orb.: orbital; Palat.: palatine; Perp.: perpendicular; Post.: posterior; Proc.: process; Pteryg.: pterygoid; Pterygomax.: pterygomaxillary; Pterygopal.: pterygopalatine; Sphen.: sphenoidal; Sup.: superior; Supraorb.: supraorbital; Troch.: trochlear; Tuberc.: tuberculum; Zygo.: zygomatic; Zygomaticofac.: zygomaticofacial; Zygomatico-orb.: zygomatico-orbital.
Another small depression in the anteromedial part of the roof, the trochlear fossa, serves as the attachment for the trochlea of the superior oblique muscle. The floor of the orbit is formed by the orbital plate of the maxilla, the orbital surface of zygomatic bone, and the orbital process of the palatine bone. The orbital floor, which is very thin, forms the roof of the maxillary sinus. The floor is continuous with the medial wall, except in the most anterior part, where the floor is perforated by the nasolacrimal canal. The anterior part of the floor is continuous with the lateral wall, but posteriorly, the floor and lateral wall are separated by the inferior orbital fissure. The infraorbital groove, which transmits the infraorbital branch of the maxillary nerve, leads forward out of the inferior orbital fissure to cross the floor to reach the infraorbital canal, which ends below the lower orbital rim in the infraorbital foramen. The lateral wall consists predominantly of the greater sphenoid wing and the frontal process of the zygomatic bone. The greater sphenoid wing also forms much of the middle fossa floor and the roof of the infratemporal fossa. Superiorly, the anterior part of the lateral orbital wall is continuous with the roof, but the posterior part of the lateral wall is separated from the roof by the superior orbital fissure.
The lacrimal foramen, which transmits the recurrent meningeal branch of the ophthalmic artery, is located anterior to the superior orbital fissure along the superior edge of the lateral wall. The zygomatico-orbital foramina on the anterolateral part of the intraorbital surface of the lateral wall transmits the zygomaticofacial and zygomaticotemporal nerves, which exit the external surface of the zygoma at the zygomaticofacial and zygomaticotemporal foramina to reach the skin of the cheek and temple. The medial wall is formed, from anterior to posterior, by the frontal process of the maxilla, the lacrimal bone, the orbital plate of the ethmoid bone, and the body of the sphenoid bone. The medial wall is extremely thin, especially in the area of the orbital plate of the ethmoid bone, which separates the orbit and ethmoid air cells. The lacrimal sac, which sits in the lacrimal groove formed by the frontal process of the maxilla anteriorly and the lacrimal bone posteriorly, opens into the nasal cavity through the nasolacrimal canal. The anterior and posterior ethmoidal foramina, which transmit the anterior and posterior ethmoidal branches of the ophthalmic artery and the nasociliary nerve, are located at the junction of the roof and medial wall of the orbit and pass through the frontoethmoidal suture or the adjacent part of the frontal bone and open into the anterior cranial fossa along the lateral edge of the cribriform plate.
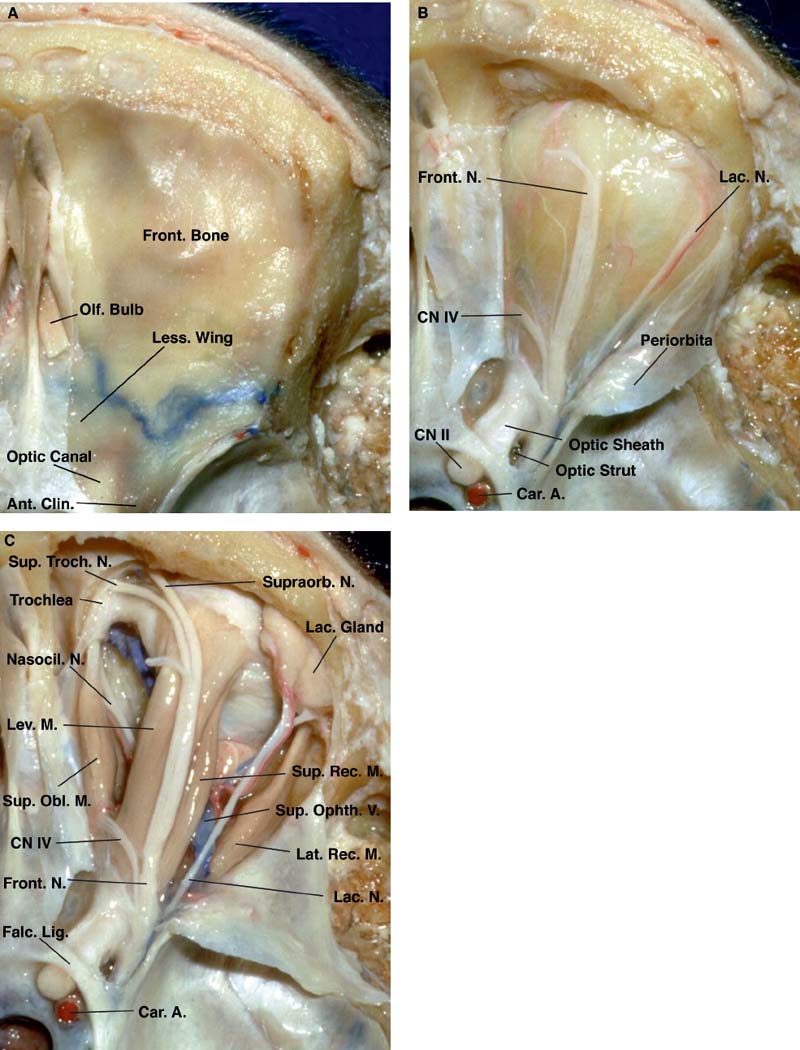
Fig. 15.2 Superior view of a stepwise dissection of the neural structures in the orbit and superior orbital fissure. (A) The dura has been removed from the part of the frontal and sphenoid bones forming the orbital roof. (B) The orbit and optic canal have been unroofed, the anterior clinoid process removed, and the periorbita opened to expose the trochlear, frontal, and lacrimal nerves coursing in the orbital fat just beneath the periorbita. (C) The orbital fat has been removed.
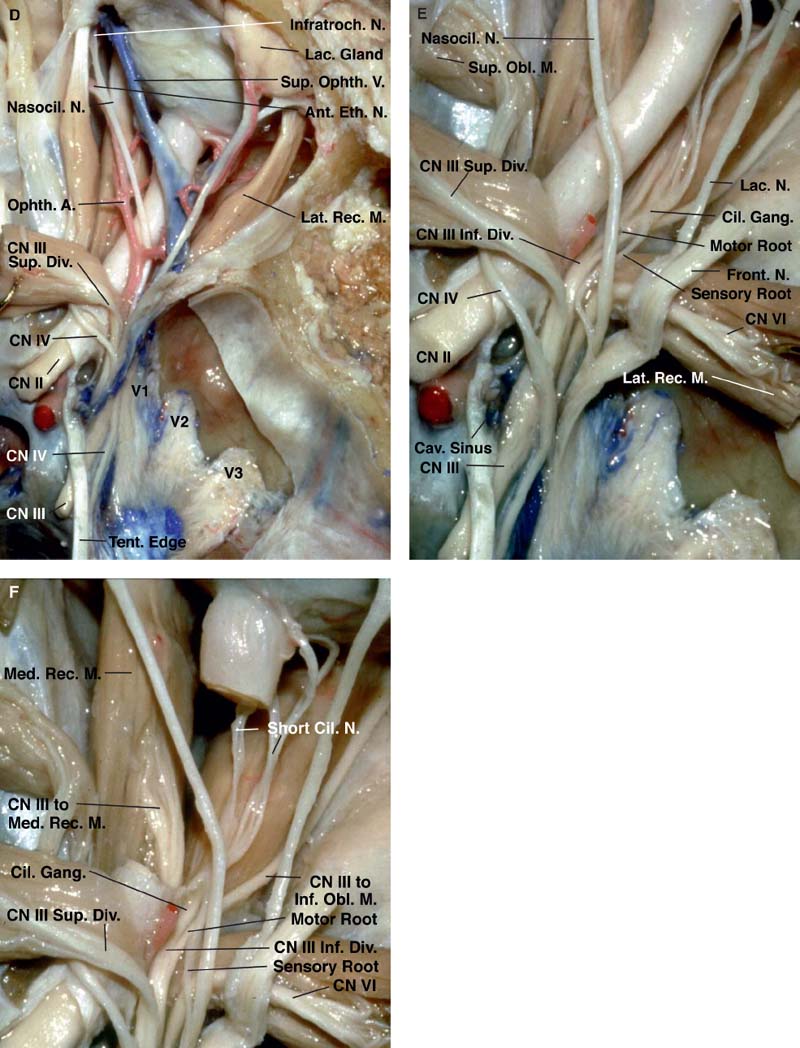
Fig. 15.2 (D) The frontal nerve and the levator and superior rectus muscles have been divided and reflected to expose the superior ophthalmic vein, ophthalmic artery, and nasociliary nerve as they pass above the optic nerve. (E) The annular tendon has been divided in the interval between the origin of the superior and lateral rectus muscles. (F) A segment of the orbital portion of the optic nerve has been removed. This exposes the branch of the inferior division of the oculomotor nerve, which passes below the optic nerve and enters the medial rectus muscle. A.: artery; Ant.: anterior; Car.: carotid; Cav.: cavernous; Cil.: ciliary; Clin.: clinoid; CN: cranial nerve; Div.: division; Eth.: ethmoidal; Falc.: falciform; Front.: frontal; Gang.: ganglion; Inf.: inferior; Infratroch.: infratrochlear; Lac.: lacrimal; Lat.: lateral; Less.: lesser; Lev.: levator; Lig.: ligament; M.: muscle; Med.: medial; N.: nerve; Nasocil.: nasociliary; Obl.: oblique; Olf.: olfactory; Ophth.: ophthalmic; Rec.: rectus; Sup.: superior; Supraorb.: supraorbital; Sup. Troch.: supratrochlear; Tent.: tentorial; Troch.: trochlear; V.: vein.
The optic canal, through which the optic nerve and ophthalmic artery pass, opens into the superomedial corner of the orbital apex at the junction of the roof and medial wall. The optic canal is situated at the junction of the lesser wing with the body of the sphenoid bone. It is separated from the superior orbital fissure by the optic strut, a bridge of bone, also referred to as the posterior root of the lesser wing, which extends from the lower margin of the base of the anterior clinoid process to the sphenoid body. The tendinous ring (annular tendon) from which the superior, inferior, medial, and lateral rectus muscles arise is attached to the upper, lower, and medial margin of the optic canal. The anterior clinoid process projects backward from the lesser wing of the sphenoid bone into the interval between where the optic nerve enters the optic canal and where the oculomotor nerve enters the superior orbital fissure. The intracranial end of the optic canal has an ovoid shape with a slightly greater diameter in the mediolateral than in the superior-inferior dimension. It is situated medial to the anterior clinoid process and optic strut.
The medial margin is formed by the body of the sphenoid bone. The upper margin is formed by the anterior root of the lesser wing of the sphenoid bone. The lateral margin is formed by the optic strut. The lower margin of the foramen is formed by the optic strut and the adjacent part of the body of the sphenoid bone. The optic strut blends superolaterally into the base of the anterior clinoid process and inferiorly and medially into the body of the sphenoid bone. The anterior bend of the intracavernous segment of the internal carotid artery rests against the posterior surface of the optic strut and ascends on the medial side of the anterior clinoid process. The body of the sphenoid bone contains the sphenoid sinus. The chiasmatic sulcus is a shallow groove situated on the intracranial surface of the sphenoid formed by the lateral surface of the optic strut, and the lower part is formed by the body of the sphenoid bone. The anterior part of the carotid sulcus, the shallow groove marking the course of the intracavernous segment of the carotid artery, is situated just inside and behind the medial edge of the fissure and continues upward along the posterior margin of the optic strut and the medial side of the anterior clinoid process. The lower margin of the fissure is formed by the junction of the greater wing with the sphenoid body and is located at the level of the lower edge of the cavernous sinus and the floor of the middle fossa. The lower edge of the fissure is separated from the foramen rotundum by a narrow bridge of bone, referred to as the maxillary strut. The lower end of the superior orbital fissure is located above and blends into the medial end of the inferior orbital fissure. The inferior orbital fissure is a narrow crevasse with long anterior and posterior borders and narrow medial and lateral ends. The long posterior edge is formed by the greater wing of the sphenoid bone. The long anterior wall is formed by the orbital surface of the maxilla, except for a short segment formed by the orbital process of the palatine bone. The narrow lateral end is formed by the zygomatic bone, and the narrow medial end is formed by the sphenoid body. The posteromedial part of the fissure communicates below with the pterygopalatine fossa and the anterolateral part communicates with the infratemporal fossa, which is located below the greater sphenoid wing. The structures passing through the fissure are the zygomatic and the infraorbital and zygomatic branches of the maxillary nerve, some branches of the internal maxillary artery, and the branches of the inferior ophthalmic vein, which communicate with the pterygoid plexus. The orbital smooth muscle spans the upper part of the fissure. The pterygomaxillary fissure is the narrow cleft between the posterior surface of the maxilla and the anterior surface of the pterygoid process of the sphenoid bone. The pterygomaxillary fissure opens into the pterygopalatine fossa, which is located below and communicates through the medial part of the inferior orbital fissure with the orbital apex. The upper part of the pterygoid process is penetrated by the foramen rotundum, through which the maxillary nerve passes to reach the pterygopalatine fossa, where it gives rise to the infraorbital and zygomatic nerves, which course in the floor and lateral orbital wall. The ostium of the vidian canal, which transmits the vidian nerve, is located below the foramen rotundum. The medial wall of the pterygopalatine fossa is formed by the perpendicular plate of the palatine bone.
 Periorbita, Dura, and Annular Tendon
Periorbita, Dura, and Annular Tendon
At the superior orbital fissure, the dura covering the middle fossa and cavernous sinus blends into the periorbita of the orbital apex and into the annular tendon from which the recti muscles arise (Fig. 15.3). The annular tendon surrounds the orbital end of the optic foramen and the adjacent part of the superior orbital fissure. The fibrous components, which blend together to form the annular tendon, are the periorbita covering the orbital apex, the dura lining the superior orbital fissure and optic canal, and the optic sheath. The annular tendon is attached along the upper, medial, and lower margins of the optic canal, and to a bony prominence at the midportion of the lateral edge of the superior orbital fissure, at the junction of the fissure’s narrow lateral and larger medial parts. The annular tendon does not surround the whole superior orbital fissure, but encompasses only the upper-medial portion, which is situated lateral to the optic strut and optic foramen. The lower portion of the annular tendon, the site of origin of the inferior rectus muscle, extends horizontally from the sphenoid body below the optic strut and optic foramen to an attachment on the lateral edge of the fissure.
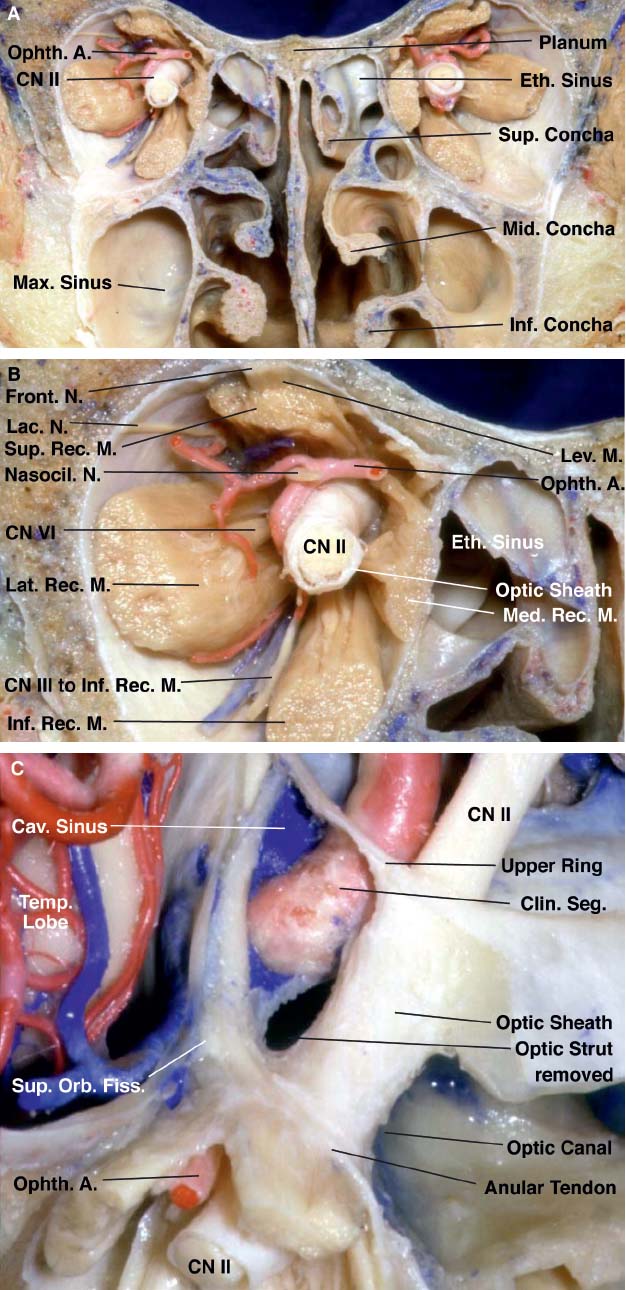
Fig. 15.3 (A) Coronal section of orbits and cranial base anterior to the orbital apex. (B) Enlarged view of right side shown in A. (C) Anterosuperior view showing the relationship of the orbital apex to the optic strut, optic canal, and superior orbital fissure.
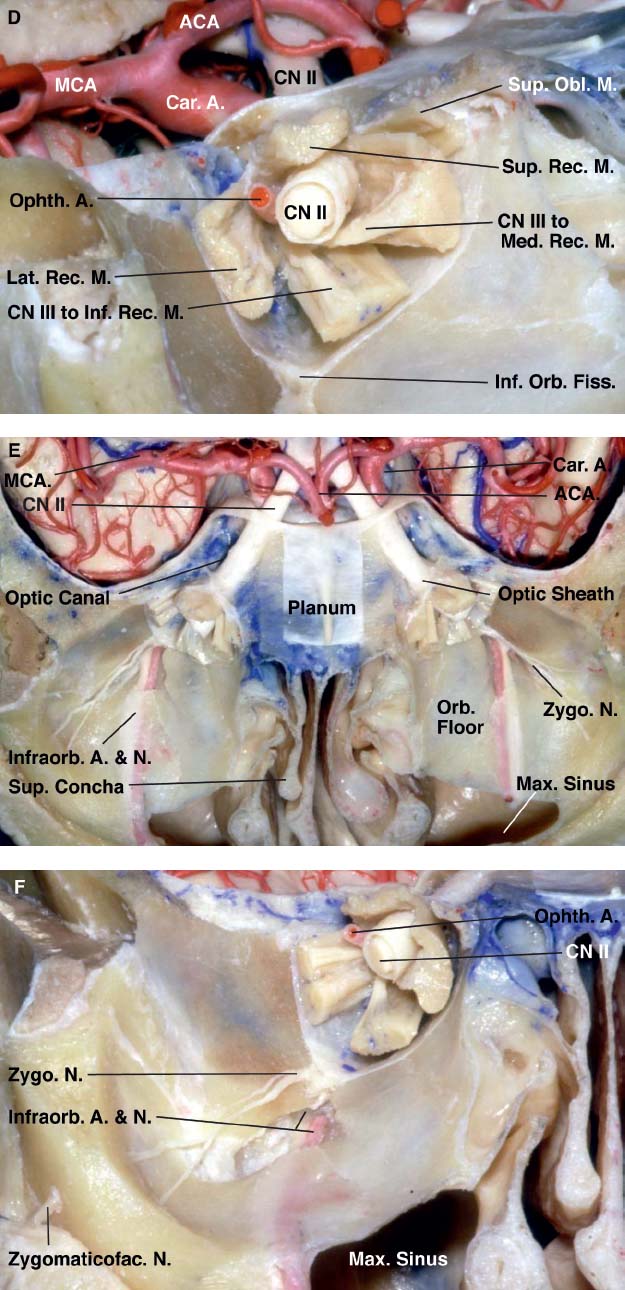
Fig. 15.3 (D) Cross section of right orbit just in front of the orbital apex. (E) Superior view of the floor of both orbits. The roof of the maxillary sinus forms the orbital floors. (F) Enlarged view of the right orbit showing the course along the orbital walls taken by the zygomaticofacial, zygomaticotemporal, and infraorbital nerves.
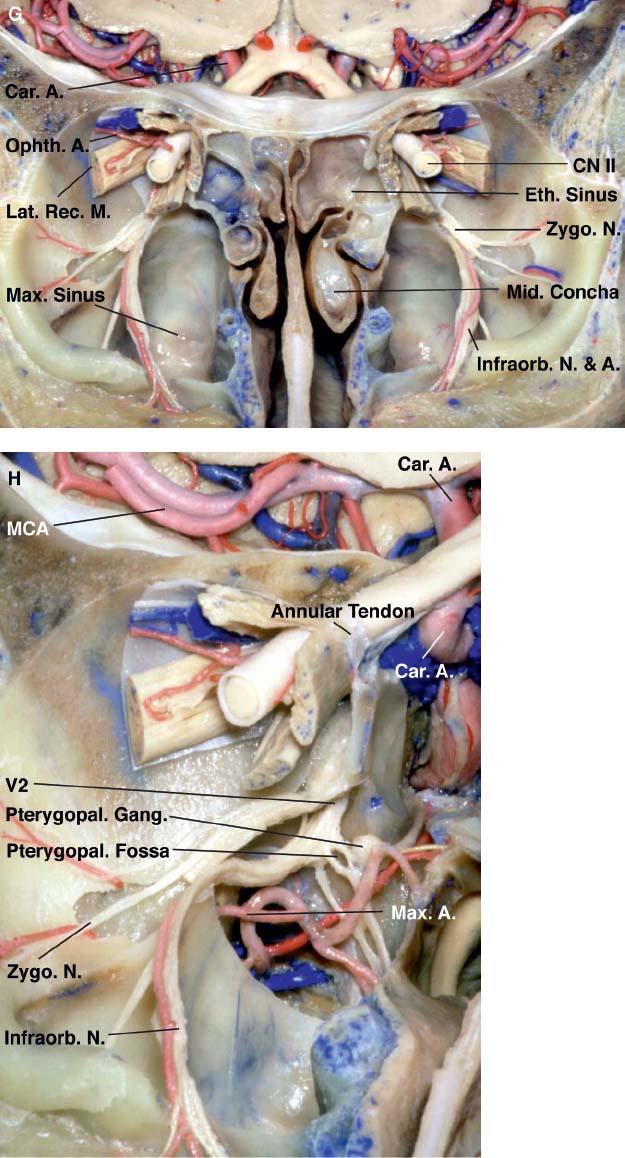
Fig. 15.3 (G) Anterior view of both orbits in another specimen. A portion of the floor of both orbits has been removed to expose the maxillary sinus while preserving the infraorbital and zygomatic nerves. (H) Enlarged view. Some of the posterior wall of the maxillary sinus has been removed to expose the pterygopalatine fossa and the origin of the infraorbital and zygomatic nerves from the maxillary nerve. A.: artery; ACA: anterior cerebral artery; Car.: carotid; Cav.: cavernous; Clin.: clinoid; CN: cranial nerve; Eth.: ethmoid; Fiss.: fissure; Front.: frontal; Gang.: ganglion; Inf.: inferior; Infraorb.: infraorbital; Lac.: lacrimal; Lat.: lateral; Lev.: levator; M.: muscle; Max.: maxillary; MCA: middle cerebral artery; Med.: medial; Mid.: middle; N.: nerve; Nasocil.: nasociliary; Obl.: oblique; Ophth.: ophthalmic; Orb.: orbital; Pterygopal.: pterygopalatine; Rec.: rectus; Seg.: segment; Sup.: superior; Temp.: temporal; Zygo.: zygomatic; Zygomaticofac.: zygomaticofacial.
From its attachment to the greater wing, the annular tendon is directed upward to blend into the periorbita and dura, which meet on the lower margin of the lesser sphenoid wing. The segment of the annular tendon passing from the greater to the lesser wing separates the narrow lateral part of the fissure from the larger medial part and serves as the site of origin of the lateral rectus muscle. The annular tendon and the connective tissue layer extending backward divide the superior orbital fissure into three sectors: lateral, central, and inferior. The lateral sector is quite narrow, being bounded above by the lesser wing of the sphenoid bone, below by the part of the greater wing lateral to the site of attachment of the annular tendon, and medially by the annular tendon and the origin of the lateral rectus muscle.
The lateral sector transmits the trochlear, frontal, and lacrimal nerves, all of which pass through the fissure outside the annular tendon. The lacrimal nerve occupies the most lateral part of the fissure; the frontal nerve is more medial. The trochlear nerve passes through the fissure on the superomedial margin of the frontal nerve. The superior ophthalmic vein also passes through this sector by coursing along the lower side of the lacrimal and frontal nerves to reach the cavernous sinus. The central sector of the superior orbital fissure, referred to as the oculomotor foramen because it is the part of the fissure through which the oculomotor nerve passes, is bounded above by the annular tendon and the adjacent part of the lesser wing, medially by the optic strut and sphenoid body, laterally by the annular tendon and the prominence on the lateral margin of the fissure to which the annular tendon attaches, and below by the segment of the annular tendon spanning the interval between the sphenoid body and the bony prominence on the lateral edge of the fissure. The inferior rectus muscle arises from the annular tendon at the lower margin of this sector. The oculomotor, nasociliary, and abducens nerves and the sensory and sympathetic roots of the ciliary ganglion pass through this sector. The optic nerve and ophthalmic artery pass medially to the oculomotor foramen through the part of the annular tendon attached to the upper, lower, and medial margins of the optic foramen. The connective tissue membrane, which extends posteriorly from the annular tendon, separates the nerves passing through the lateral and central sectors of the fissure. This connective tissue extends backward from the annulus between the frontal branch of the ophthalmic nerve, which passes through the lateral sector outside the annular tendon, and the nasociliary nerve, which passes through the central sector and the annular tendon.
The inferior sector of the superior orbital fissure is situated below the annular tendon. It is bounded below by the junction of the body and greater wing of the sphenoid bone, above by the annular tendon, laterally by the part of the greater wing below the attachment of the annular tendon, and medially by the sphenoid body. The inferior rectus muscle arises from the annular tendon at the upper margin of this sector. Orbital fat extends backward below the inferior rectus muscle into this part of the fissure. The lower margin of this sector contains a posterior extension of the orbital smooth muscle, which spans the upper margin of the inferior orbital fissure. The orbital fat extends backward between the inferior rectus muscle and the orbital smooth muscle and medial to the segment of the abducens and nasociliary nerves passing through the fissure. Removal of this fat exposes the fine branches of the carotid sympathetic plexus entering the orbit, some of which form the sympathetic root of the ciliary ganglion.
 Neural Relationships
Neural Relationships
Optic Nerve
The optic nerve is divided into four parts: intraocular, intraorbital, intracanalicular, and intracranial (Figs. 15.2, 15.3, 15.4, and 15.5). The intracanalicular part, located in the optic canal, and the intraorbital portions of the optic nerve are surrounded by dura and arachnoid. The subarachnoid space surrounding the intracranial part of the nerve extends forward from and communicates with the subarachnoid space around the intracanalicular and intraorbital portions of the nerve. The optic nerve passes through the medial part of the annular tendon and below the levator and superior rectus muscles. The dural sheath around the optic nerve blends smoothly into the periorbita at the anterior end of the optic canal. After passing through the optic canal, which forms a prominence in the upper part of the sphenoid sinus immediately in front of the sella turcica and along the medial aspect of the anterior clinoid process, the intracranial portion of the nerve is directed posterior, superiorly, and medially toward the optic chiasm. The intraocular portion of the optic nerve, which includes the optic disc, lies within the sclera. The intraorbital portion of the optic nerve is surrounded by orbital fat and follows a slightly tortuous course. The ciliary nerves and arteries pierce the sclera in the area around the optic nerve. The ophthalmic artery enters the orbit on the lateral side of the nerve and passes above the nerve to reach the medial sides of the orbit. The superior ophthalmic vein arises in the anteromedial part of the orbit and crosses above the nerve to reach the orbital apex. Both the artery and vein course between the superior rectus muscle and the optic nerve. The branch of the inferior division of the oculomotor nerve to the medial rectus muscle passes below the optic nerve at about the same level that the ophthalmic artery and nasociliary nerve pass above the optic nerve.
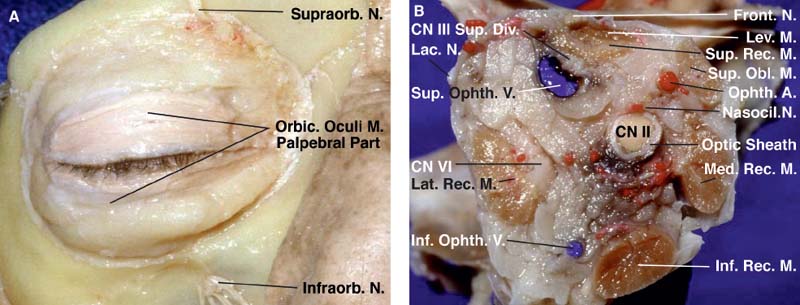
Fig. 15.4 (A) The orbital part of the orbicularis oculi muscle has been removed and the palpebral part preserved. (B-H) Anterior views of cross sections of the orbit at progressively deeper levels. (B) Anterior aspect of a coronal section through the right orbit just posterior to the globe and the inferior oblique muscle.
Related posts:
 Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Combined Cranio-Endoscopic Approach
Endoscopic Transethmoid-Pterygoid-Sphenoid Approach
Anesthesia in Endoscopic Skull Base and Brain Surgery
The Endonasal Transplanum-Transtuberculum Endoscopic Approach in Pituitary Adenomas
Endoscopic Transnasal Craniectomy and the Resection of Extensive Craniopharyngiomas
External Versus Endoscopic Approaches for Skull Base Malignancies
Combined Cranio-Endoscopic Approach
Endoscopic Transethmoid-Pterygoid-Sphenoid Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


