1.D. All three are mechanisms of antiacetylcholine receptor antibodies. 2.B. The medial lemniscus (ML) is widely separated from the anterolateral system (ALS) in the medulla. In fact, ML and ALS fibers receive different blood supplies in the medulla. In the midbrain and pons, the ML and ALS are in close proximity and receive similar blood supplies. 3.E. Sodium hydroxide (2N) for 1 hour is the current standard for decontamination after CJD cases. Characteristic features of CJD include ataxia, myoclonus, and dementia. Death usually occurs within 1 year after onset of symptoms. 4.A. McRae’s line is from the basion to the opisthion. 5.C. It is helpful to remember that this pattern of somatotopy can be appreciated in the descending motor pathways: those tracts that are concerned with flexor musculature (corticospinal tract and rubrospinal tract) lie dorsal to those tracts concerned with extensor musculature. 6.D. All tissues increase oxygen extraction in the face of decreased blood flow except the coronary circulation, which is flow dependent. 7.A. Rhinocerebral mucormycosis on pathology reveals pleomorphic short and wide nonseptate hyphae. It can be treated with Cancidas, Voriconazole, and AmBisome. It may cause hemorrhagic necrosis and ischemic strokes. The organism originates in the soil. 9.C. Cerebral ischemia begins when CPP falls below 50 mm Hg. 10.B. The clinoidal triangle is defined by the medial border of the optic nerve and the oculomotor nerve laterally. 11.E. Dysphagia in myasthenia gravis is fatigable, and the patient often relates a history of little difficulty with breakfast, moderate difficulty with lunch, and inability to eat in the evening. 12.E. Skin changes precede muscle abnormalities in dermatomyositis (DM). Polymyositis (PM) is diagnosed by fibrillation potentials on EMG and elevated CPK (creatine phosphokinase) levels (higher than DM). In polymyositis, there is widespread single-fiber necrosis and T cells with macrophages may be found in the muscle fibers. PM is the most frequent inflammatory myopathy. 13.E. Protein 14–3-3 is elevated in the CSF with destructive diseases of the CNS. This protein is sensitive for Creutzfeldt-Jakob disease, but not specific. 14.B. The posterior cord gives rise to the axillary nerve and the radial nerve as its terminal branches. 16.D. Increased dead space is caused by overdistended alveoli (COPD and PEEP), or by decreased blood flow (CHF, pulmonary embolus, emphysema). 17.D. After basilar skull fractures, the most common pathogen is S. pneumoniae, and the infection usually occurs within the first few days. 18.D. 19.E. General treatment of ICP is aimed at minimizing these factors. 20.C. 21.B. 22.E. Weber’s syndrome involves the base of the midbrain. It is characterized by CN III palsy with crossed hemiplegia. All other syndromes mentioned may have ataxia as part of the clinical findings. 23.A. 24.C. Lesions of the DM thalamus, hippocampus, or temporal cortex cause memory impairment. 25.B. The x-ray shows a cervical rib, usually associated with ulnar nerve weakness and paresthesia, Raynaud’s syndrome, and traction meningocele. 26.A. Positive end-expiratory pressure (PEEP) decreases the work of breathing and the FIO2 requirement, but it may decrease cerebral perfusion pressure. PEEP increases the physiologic dead space, lung compliance (therefore, decreasing plateau pressure), and risk of barotrauma. 27.E. None of these maneuvers actually reduces infection rate. 28.B. Serotonin pathways inhibit copulation, explaining the side effect of decreased libido with selective serotonin reuptake inhibitors (SSRIs) used to treat depression. Administration of L-dopa increases libido. Noradrenergic receptors in the brain exert an inhibitory effect on penile erection. 30.D. Parkinson’s (infratrochlear) triangle is located between the lower margin of the trochlear nerve and the upper margin of the opthalmic nerve. 31.D. The Tensilon test is sensitive in diagnosing a defect in neuromuscular transmission, but is not specific for myasthenia gravis (MG). The Tensilon test is especially useful in ocular MG, when other diagnostic tests may be negative. Depending on the mechanism of AchR antibodies, there may be insufficient numbers of AchRs available so that a negative Tensilon test does not negate the diagnosis of MG. There is no correlation between the results of the Tensilon test and the subsequent response to pyridostigmine. 32.D. The posterior interosseous nerve (C7, C8) is a branch of the radial nerve. The posterior interosseous nerve innervates the extensor digitorum, extensor digiti minimi, and the extensor carpi ulnaris. The extensor carpi ulnaris extends the hand at the wrist joint. This muscle is spared in posterior interosseous syndrome. 33.A. The Nernst equation describes the membrane potential produced by a concentration of a diffusible ion across a membrane. E is the voltage produced, R is the gas constant, T is the absolute temperature, z is the ionic charge, F is Faraday’s constant, and Q is the ratio of the concentrations on the two sides of the membrane. 35.D. Ocular myoclonus is a pendular vertical oscillation of the eyes, usually of large amplitude and often occurring with movements of the palate. It can develop months to years after bilateral destructive lesions of the central tegmental tract and is often accompanied by bilateral horizontal gaze palsies. 36.A. Early hypoxemia characterizes ARDS. 37.C. Maximum collagen deposition occurs at 42 days (~6 weeks). Tensile strength keeps on increasing until 2 years. 38.B. Rosenthal fibers are by no means a requisite feature of pilocytic astrocytoma. Rosenthal fibers are composed of alphaB cystallin and are surrounded by intermediate filaments. 39.E. Barbiturates are also thought to stabilize lysosomes, suppress the formation of edema, and reduce intracellular accumulation of calcium. The inverse steal phenomenon involves barbiturate-induced vasoconstriction resulting in shunting of blood from normal brain to relatively ischemic areas. 40.E. 41.C. The majority of AchR antibodies are immunoglobulin G (IgG). Cyclosporine should be used if first-line treatments have failed. Pathologic abnormalities of the thymus occur in up to 80% of patients. Weakness confined to the ocular muscles for over 3 years suggests good prognosis. 42.D. 44.B. The most accurate description of Wernicke’s area is that it includes the supramarginal (39), angular (40), and posterior one third of the superior temporal gyri. 45.A. Bursts of back-to-back saccades seen in opsoclonus and ocular flutter may be attributable to a disorder of pause cell modulation of burst cell function. 46.C. 47.A. Scan 1 shows a glomus tympanicum tumor which may be associated with 48.B. catecholamine release causing hypertension, or serotonin and kallikrein 49.A. release causing bronchoconstriction, abdominal pain, and diarrhea. 50.A. Glomus tympanicum tumors may also release histamine and bradykinins 51.D. during surgery, causing hypotension and bronchoconstriction. Scan 2 shows a meningioma of the cerebellopontine angle (CPA), which usually presents initially with facial nerve involvement. Acoustic schwannomas present initially with hearing loss and tinnitus. 52.A. Disseminated intravascular coagulation is most frequently associated with obstetric catastrophes, metastatic malignancy, massive trauma, and bacterial sepsis. The neurosurgeon should be aware that DIC can occur when there is major cerebral tissue injury. The decrease in fibrinogen most closely correlates with increased bleeding. Treatment is aimed at reversing the causative agent, and transfusing heparin, cryoprecipitate, platelets, and/or whole blood. 53.C. The mastoid air cells and the posterior middle fossa are innervated by V3. The supratentorial compartment is innervated by V1 and V2. The infratentorial compartment is innervated by IX, X, and C1–3 posterior roots. 54.D. The band of Gennari divides the fourth layer of cortex into two granular layers with a thick myelin layer. The band is located only in area 17 (primary visual cortex, also known as V1). When Gennari described this in 1782, he had no idea that this region might be concerned with vision. 56.C. Climbing fiber input is most active at times when the subject is performing new complex movements. The climbing fiber input can modify the synapse between the parallel fiber (from the granule cell) and the Purkinje cell. 57.D. The combination of high trophic hormone and low target hormone indicates target gland failure. 58.D. The opponens pollicis inserts on the first metacarpal bone. 59.A. Resolution of brain edema occurs mainly through bulk flow into the CSF. 60.B. 61.C. 62.A. 63.E. 64.D. 65.C. The MLF is responsible for the binocular coordination of all categories of horizontal, vertical, and oblique eye movements with the exception of vergence movements. Nystagmus on upgaze is a feature of MLF lesions. 66.C. Both Apert’s and Crouzon’s syndromes are autosomal dominant (both may also be sporadic). Both are associated with bilateral coronal synostosis. Those with Apert’s syndrome manifest more severe mental retardation than patients with Crouzon’s syndrome. 67.E. In addition to stimulating the synthesis and secretion of TSH, TRH is a potent secretagogue for prolactin, and to a lesser extent ACTH and GH. 68.C. The metacarpophalangeal joint of the ring finger is flexed by the lumbrical, palmar, and dorsal interosseous muscles, which are innervated by the ulnar nerve. The joint is extended by the extensor digitorum, which is innervated by the radial nerve. The median nerve is mainly involved with flexion of the ring finger. 69.C. Interstitial edema is a feature of hydrocephalus. 70.D. 71.E. Serum concentration of PRL is increased after tonic clonic seizure activity, but not affected by nonepileptic seizures. 73.A. The sinuvertebral nerve arises just distal to the dorsal root ganglion. The posterior disk receives its innervation from the sinuvertebral nerves. The anterior disk receives its innervation from the gray rami communicans. 74.B. Repetition is impaired in conduction aphasia. 75.B. The usual diameter of the internal cerebral artery at the clinoid area is ~8 mm. This aneurysm is slightly smaller than the artery’s diameter. 76.B. The greatest threat to the patient’s life during surgery for craniosynostosis is blood loss and hypothermia. 77.B. 78.C. The medial brachial cutaneous nerve (from the medial cord) contains sensory fibers that have cell bodies in the dorsal root ganglia. It also contains sympathetic postganglionic fibers that have cell bodies in the sympathetic chain ganglia. 79.B. The perforant path is the main excitatory pathway to the hippocampus. When perforant path fibers are stimulated, histological changes develop in the pyramidal nerve cells of CA1 and CA3. 80.C. 81.B. Up to 80% of the population will experience a tension headache in their lifetime. Amitriptyline is the most effective medication used to prevent tension headaches. 82.C. The ambient cistern contains the trochlear nerve. 83.B. The anterior and medial scalene muscles insert onto the first rib, and the subclavian artery, subclavian vein, and brachial plexus pass between them. 84.A. Pure word blindness is characterized by alexia without agraphia. The patient is unable to read, but is able to understand speech, write, and speak. It is caused by a lesion of the left geniculocalcarine tract and the corpus callosum. 85.C. Preventing seepage of blood into the ventricular system during a hemispherectomy is accomplished by obstructing the foramen of Monro and maintaining the integrity of the septum pellucidum. 87.D. Sexual precocity is often the presenting symptom of hypothalamic hamartomas. Hypothalamic hamartomas may also cause gelastic (laughing) seizures. 88.D. Pleomorphic xanthoastrocytoma (PXA) is an astrocytic neoplasm with a relatively favorable prognosis. 89.B. Excitatory input from CA3 to CA1 pyramidal cells is carried by Schaffer collaterals. These collaterals spare the CA2 region. 90.B. 91.A. The amino acids phenylalanine and tyrosine are precursors for catecholamines (dopamine, norepinephrine, epinephrine). 92.D. The gracile and cuneate fasciculi are supplied by the posterior spinal arteries. The paired posterior spinal arteries [arising from either posterior inferior cerebellar artery (PICA) or vertebral] supply the posterior one third of the spinal cord. 93.C. Adson’s test is used in the examination of thoracic outlet syndrome. In this example the examiner is checking to see if the radial pulse is obliterated. Compression of nerves causes wasting of muscles supplied by the lower trunk of the brachial plexus. 94.E. The corticobulbar tract is located in the genu of the internal capsule. 95.D. The medial forebrain bundle traverses the entire lateral hypothalamic area and interconnects the septal area and nuclei, the hypothalamus, and the midbrain tegmentum. The medulla is connected with the hypothalamus via the dorsal longitudinal fasciculus, which projects to the parasympathetic nuclei of the brainstem. 96.D. It is postulated that the closure of the lambdoid sutures, common in Crouzon’s syndrome, results in cerebellar tonsillar herniation. 97.A. The most severe forms of hypothalamic cachexia are seen in lesions of the lateral hypothalamus. 99.B. Bcl-2 is an inhibitor of apoptosis similar to Ced-9 in C. elegans. HSP (heat shock proteins) are related to the cell’s ability to withstand thermal stress. 100.D. Renal cell carcinoma has a predilection for the ventricular system. 101.A. Ireland has the highest incidence of PKU (1 in 5000). PKU is caused by a deficiency in phenylalanine hydroxylase, which has significantly reduced levels of enzyme activity. This results in abnormally high levels of phenylalanine with diminished levels of tyrosine. An accumulation of phenylalanine can result in brain damage with features including mental retardation, seizures, and aggressive tendencies. 102.B. The straight sinus is formed by the great cerebral vein of Galen and the inferior sagittal sinus. 103.D. Oscillopsia is a condition where objects seem to wiggle; it sometimes accompanies downbeat nystagmus. 104.A. Atropine only blocks muscarinic receptors, thus only preganglionic synapses are affected. 105.A. Wernicke’s encephalopathy is due to deficiency of thiamine (B1). 106.D. Gustatory fibers of the solitary nucleus terminate in the VPM, while fibers carrying thoracic information terminate in the parabrachial nucleus and hypothalamus. 107.B. In contrast to diffuse astrocytomas, anaplastic astrocytomas typically display mitotic activity. 108.D. The typical site for a cavernous hemangioma of the orbit is in the intraconal space lateral to the optic nerve. 109.C. This EKG demonstrates J-point elevation, which is associated with hypothermia. 110.E. Small arteries from the ependymal surface feed the AVM. 112.B. The venous angle is a landmark for the foramen of Monro. It is formed by the union of the septal vein and the terminal (also called thalamostriate) vein. 113.E. Ocular bobbing is a rapid downward movement of the eyes with a slow return to midposition and has many causes. 114.E. This CT reveals dense sclerosis around a lytic lesion with a central calcified nodule in the lumbar neural arch. 115.C. The striae medullares (rhombencephali) arise from the arcuate nuclei of the medulla and are seen on the floor of the rhomboid fossa. These fibers divide the rhomboid fossa into a rostral pontine half and a caudal medullary half. The stria medullaris (thalami) contains septohabenular fibers. The stria terminalis is a semicircular fiber bundle extending from the amygdala to the hypothalamus and septal area. 116.C. No blood vessels penetrate the intervertebral disc. Delivery of nutrients is entirely dependent on diffusion. 117.D. The olivocochlear bundle arises from the region of the superior olivary nucleus and projects contralaterally back to the hair cells of the cochlea. Stimulation of this bundle results in inhibition or reduction of responses of auditory signals by auditory nerve fibers. 118.B. Pleomorphic adenomas of the lacrimal gland should be removed with a cuff of normal tissue to reduce the risk of tumor seeding and recurrence. An incisional biopsy should not be performed on this type of tumor. 119.C. 120.C. 121.B. Dopa-responsive dystonia (Segawa’s syndrome) is due to a mutation in the gene encoding guanosine triphosphate (GTP)-cyclohydrolase 1, the rate-limiting enzyme in the synthesis of the biopterin cofactor of tyrosine hydroxylase. Tyrosine hydroxylase requires a biopterin cofactor and iron for proper functioning. This condition is autosomal dominant and begins in the first decade of life with a marked diurnal variation of a lower limb dystonia. 123.D. In the comatose patient, a lesion at the level of the vestibular nuclei results in extensor movements of the arms and weak flexor movements of the legs. Flaccidity of the lower and upper extremities occurs with lesions below the vestibular nuclei. Lesions above the red nucleus (decorticate) result in flexion of the upper and extension of the lower extremities. Lesions below the red nucleus (and above the vestibular nuclei) result in extensor posturing of all extremities (decerebrate). 124.E. Fibers of the chorda tympani reach the sphenopalatine ganglion to produce “crocodile tears,” also known as Bogorad’s syndrome. 125.A. With a cervical syrinx, one would expect attenuation or abolition of the cervical N13 evoked potential. N13 attenuation may be due to involvement of those laminae of the dorsal horn that receive input from large-diameter mechanoreceptor fibers. 126.C. Wolff’s law states that a bone develops the structure most suited to resist the forces acting upon it. Sherrington’s law: every posterior spinal nerve supplies a special region of skin. Jackson’s law: the nerve functions that are latest developed are the first to be lost. Delpech’s principle: in spondylolisthesis, when slippage reaches around 30% the anterior inferior part grows at a faster rate than the overloaded posterior part of the vertebral body. 127.D. Chordomas tend to be in the midline, while chondrosarcomas are more frequently found off the midline (at the petrosphenoid synchondrosis). Chordomas express S-100 only variably. Normal neurologic examinations are more common in patients with chordoma, whereas visual loss, facial numbness, and multiple cranial neuropathies are more common in patients with chondrosarcoma. These differences probably reflect the tendency of chordomas to originate from the clivus and chondrosarcomas from the temporal bone. 128.A. Thalamotomy is quite effective for medically refractory essential tremor. The patients who benefit most from thalamotomy are usually young with tremor-predominant Parkinson’s disease. 129.D. Due to considerable variation in the attachment of the dentate ligament, the best estimate of the equator is the midway point of the dorsal and ventral rootlets. The equator is a useful landmark for the posterior extent of a cordotomy incision and marks the point of the sacral-most fibers of the spinothalamic tract. The exiting ventral roots are ~5 mm from the anterior spinal artery. 130.C. It usually takes 12 to 18 months for radiation changes to appear on MRI scans. 131.C. L-dopa is converted very quickly to dopamine by AADC. Dopamine is converted to NE by dopamine β-hydroxylase, which is found in vesicles within the catecholaminergic neuron. 132.B. 133.A. The length constant is the distance along a fiber where a change in the membrane potential produced by a given current decays to a value of approximately one third of its original value. It is directly proportional to membrane resistance and inversely related to axial resistance (the resistance of the cytoplasm within the fiber). 134.D. Raynaud’s phenomenon is caused by mast cell dysfunction; sympathectomy has not proven helpful. Half of these patients have collagen vascular disease. 135.D. Epidural hematomas are the most common intracranial hematoma in children. Although an arterial component is of major concern, diffuse oozing from the bone or from the highly vascularized periosteal surface of the dura is now considered to be a more common source of epidural hematomas in children. 136.E. Spondylolysis is a bone defect in the posterior vertebral arch between the upper and lower articular processes, that is, the isthmus or pars interarticularis. 137.B. Winged scapula is caused by paralysis of the serratus anterior muscle as a result of damage to the long thoracic nerve that arises from the roots of the brachial plexus (C5-C7). 138.A. The typical thalamotomy target is the Vim (ventralis intermedius) nucleus. Often just inserting the electrode into Vim reduces the tremor (microthalamotomy effect), and indicates that the electrode is in good position. 139.D. All are derived from the telencephalon. 140.D. 141.C. Dopamine β-hydroxylase (DBH) is released from cells when its product, norepinephrine, is released. DBH is found in the vesicles of the catecholaminergic neurons. 142.B. 144.E. The supplementary motor area (area 6) is unique because a lesion in that location is associated with no language output, usually with complete recovery in weeks to months. This is in contrast with the perisylvian language sites. 145.A. During middle fossa approaches, this anatomy can be appreciated. As the dura is elevated, branches of the middle meningeal artery are encountered and the greater and lesser superficial petrosal nerves are identified immediately posterior to the foramen spinosum. With careful bone removal, the greater superficial petrosal nerve can be traced back to the geniculate ganglion. 146.E. The position of the posterior inferior tip of L5 characterizes spondylolisthesis (III–V being higher grades). 147.D. Golgi tendon organs detect tension in the muscle fiber. Afferent signals are carried by Ib fibers to interneurons that decrease the ? motor neuron output. 148.D. The Vim is thought to be a relay nucleus for kinesthetic sensation. All observations indicate placement in the Vim. Contralateral paresthesias from stimulation of the Vim occurs at higher thresholds than those obtained from the VC nucleus (posterior to the Vim). 149.C. Glomeruli of the olfactory nerve are composed of mitral and tufted cells. Axons of mitral and tufted cells go on to form the lateral olfactory tract. 150.A. The sylvian triangle is defined angiographically by (1) the most posterior branch of the middle cerebral artery as it exits the sylvian fissure, (2) branches of superior ramifications of the MCA, and (3) inferior loops of the MCA. 151.D. MAOA and MAOB are associated with the outer mitochondrial membrane. 152.A. The metencephalon is a secondary vesicle that becomes the pons, cerebellum, and upper part of the fourth ventricle. The myelencephalon becomes the medulla and the lower part of the fourth ventricle. 153.A. The tectorial membrane is a projection of the spiral limbus that overlies hair cells of the organ of Corti. The basilar membrane supports the organ of Corti and separates the cochlear duct from the scala tympani. The vestibular membrane (Reissner’s membrane) separates the scala vestibuli from the cochlear duct. 155.C. The film shows a grade I spondylolisthesis at L4-L5. Although management of this problem is wide ranging, the best management from the choices given is a pedicle screw fusion at the concerning levels (L4-L5). 156.B. The GABA-B receptor is activated by the GABA analogue baclofen, is not chloride dependent, and is bicuculline insensitive. GABA-C is found in the retina, hippocampus, and cerebellum, and is insensitive to baclofen and bicuculline. 157.C. Structures that pass above the tendinous ring are the lacrimal nerve, frontal nerve, and CN IV (trochlear). 158.C. The most common causative organism of brain abscesses in trauma is Staphylococcus. 159.B. The most common causative organism of brain abscesses in adults due to chronic otitis is Streptococcus. 160.A. The most common causative organisms of brain abscesses in neonates are Citrobacter, Bacteroides, Proteus, and gram-negative bacilli. 161.A. Tranylcypromine is an inhibitor of MAOA. Deprenyl is a specific inhibitor of MAOB. 162.B. The floor plate contains the ventral white commissure. 163.E. Sturge-Weber syndrome occurs sporadically without mendelian inheritance and is of unknown etiology. 164.E. There are non-choroid plexus sites of CSF production. Likewise there are sites of absorption other than the arachnoid granulations (paranasal sinuses, cervical lymphatics, exiting nerve roots, and transependymal flow). 165.C. In patients with known systemic cancer, 10 to 15% of single brain lesions are cerebral abscesses or primary brain tumors. 166.A. Vigabatrin interferes with GABA breakdown, while tiagabine interferes with GABA reuptake. 167.B. 168.B. Lesions placed too laterally during thalamotomy risk injury to the internal capsule (posterior limb). Lesions placed too posterior may cause contralateral hemisensory deficits owing to injury of the VC (ventralis caudalis) nucleus. 170.E. The perforating arteries from the Pcom are termed the anterior thalamoperforating arteries. Those from the P1 are called the posterior thalamoperforating arteries. Those from P2 are termed the thalamogeniculate arteries. 171.D. 172.E. The basal plate gives rise to the hypoglossal nucleus, nucleus ambiguus, dorsal motor nucleus of the vagal nerve, and the inferior salivatory nucleus. 173.D. The clinical diagnosis of HHT is based on documentation of two of the following features: (a) recurrent epistaxis, (b) telangiectasias in areas other than the nasal mucosa, (c) autosomal-dominant inheritance, and (d) visceral involvement. 174.B. Kocher’s point places the catheter in the frontal horn of the lateral ventricle. One can measure 1 cm anteriorly to the coronal suture or 3.5 cm in front of the bregma. This precaution is to avoid the motor strip. Keen’s point would be used for placement of the catheter in the trigone and would require entrance through the posterior parietal region. 175.B. The MRI demonstrates absent flow voids in the left vertebral artery, a finding consistent with Wallenberg syndrome. 176.C. Clonazepam acts by increasing GABA-A opening frequency and does not have any hepatic enzyme-inducing properties. 177.A. 178.E. Freezing episodes and postural instability do not appear to be improved with pallidotomy. 179.E. It is bounded medially by the adductor longus. 180.C. 181.B. Serotonin is found in many cells that are not neurons, such as platelets, mast cells, and enterochromaffin cells. In fact, the brain accounts for only ~1% of body stores of serotonin. 183.A. Sneddon’s syndrome is a potentially fatal, slowly progressive, neurocutaneous disorder that affects primarily small- to medium-sized arteries. Seddon is a classification of nerve injury, and not a syndrome. 184.D. When dissecting below the arcuate line, the transversalis fascia is the only fascial layer between the rectus abdominis and the peritoneum. 185.B. Cranial neuropathies are a more common presenting sign of ependymomas than other tumors due to their tendency to arise from the floor of the fourth ventricle. Medulloblastomas typically arise from the inferior medullary velum. 186.D. Lissauer’s tract caps the dorsal horns and these fibers terminate in the substantia gelatinosa (lamina II). 187.B. The limen insula is part of the primary olfactory cortex and is found at the junction of the insular and frontal lobe cortex. 188.C. If the electrode is correctly placed, visual thresholds are usually between 2 and 3 V. Higher values indicate that the electrode is too far superior. Lower values indicate that the electrode is too far inferior. 189.C. The adductor canal contains the femoral vessels, the saphenous nerve, and the nerve to the vastus medialis. 190.B. 191.B. 192.D. 193.C. 194.B. 195.A. 196.D. Enlarged pituitary stalk may be due to sarcoidosis, which can present with elevated angiotensin converting enzyme levels. It may also be due to Langerhans cell histocytosis, which may present with eosinophilic granuloma. It can occur in cases of meningitis in children. It is very rarely associated with primary pituitary tumors. 197.D. 199.A. 200.E. 201.B. 202.E. Golgi tendon organs are sensitive to muscle tension. 203.D. 204.A. Shunt nephritis is a well-described complication of VA (ventriculoatrial) shunts. VA shunt complications are much more severe and potentially life threatening than VP shunt complications. 205.C. There is a paucity of mitoses and no necrosis in DNET. 206.D. The patient likely presents with an ACTH-secreting macroadenoma. Proper evaluation prior to surgery includes ophthalmologic and endocrine consultations and endocrine panel of laboratory tests. 207.D. 208.D. All of the information that is passed between the brainstem and the cerebellum enters and exits through one of three cerebellar peduncles: inferior cerebellar peduncle or the restiform body at the level of the medulla, middle cerebellar peduncle or the brachium pontis at the level of the pons, or superior cerebellar peduncle or the brachium conjunctivum at the level of the midbrain. The vestibulocerebellar tract traverses the juxtarestiform body. 209.C. Higher levels of TrkA are seen in neuroblastomas with favorable histology. The other factors listed are associated with worse prognosis in neuroblastomas. 211.C. Choline acetyltransferase is the definitive marker for cholinergic neurons. Hemicholinium-3 blocks the high-affinity cholinergic reuptake process. 212.A. Tanycytes are a variety of ependymal cells found in the wall of the third ventricle. The tanycyte is a cell with intermediate features between astrocytes and ependymal cells. 213.B. The diagram shown represents the lumbar plexus: structure A is the ilioin- 214.D. guinal nerve, B is the genitofemoral nerve, C is the lateral femoral cutaneous 215.E. nerve, D is the femoral nerve, and E is the obturator nerve. 216.C. 217.B. 218.B. Facial agnosia (prosopagnosia) results from bilateral damage to the medial basal occipitotemporal cortex. 219.E. All of the above may present in children with neuroblastomas. Diarrhea is from VIP secretion by the tumor. Ondine’s curse results from impaired autonomic control of respiration. 220.C. 221.D. The synthesis of NO (nitrous oxide) involves the conversion of L-arginine into NO and citrulline. All three isoforms of NOS require tetrahydrobiopterin as a cofactor and NADPH as a coenzyme. 222.B. The substantia gelatinosa (Rexed lamina II) is found at all cord levels and is homologous to the spinal trigeminal tract. It is associated with light touch, pain, and temperature sensation and it integrates input for the ventral and lateral spinothalamic tracts. 224.D. The scan demonstrates an intramedullary cavernoma. These lesions tend to bleed in patients of young age, show a clear sensory level, present with sub-arachnoid hemorrhage or by progressive ascending paraplegic syndrome. The definitive therapy is microsurgical elimination. 225.B. 226.D. 227.B. 228.D. Delta waves occur with deep sleep, infancy, and brain disease. 229.E. The stylohyoid is innervated by VII. The styloglossus is innervated by XII. The stylopharyngeus is innervated by IX. 230.E. Hyperbaric oxygen treatment is an alternative to standard surgical removal of infected bone flaps. 232.D. Clarke’s nucleus is found at the base of the dorsal horn and corresponds to Rexed VII lamina. Clarke’s column extends from C8 or T1 to about L3. Clarke’s nucleus is homologous to the accessory cuneate nucleus of the medulla. It subserves unconscious proprioception from the muscle spindles and Golgi tendon organs and is the origin of the dorsal spinocerebellar tract. 233.E. Basal encephaloceles should be treated as early as possible. Children with basal encephaloceles in the nasopharynx are at significant risk of developing meningitis. 234.B. The anterior limb of the internal capsule (on horizontal section) can be found between the caudate nucleus and the corpus striatum (globus pallidus and putamen). Clinically important tracts lie in the genu and posterior limb. The posterior limb (on horizontal section) can be found between the thalamus and the corpus striatum (globus pallidus and putamen). The posterior limb of the internal capsule contains corticospinal fibers. 235.D. 236.A. 237.B. 238.C. 239.D. The greater occipital nerve is a sensory nerve from the dorsal ramus of C2. 240.C. Thromboxane synthesis inhibitors lead to a buildup of arachidonic acid. 241.C. The lateral portion of the substantia nigra pars reticulata (SNpr) is connected with cortical and brainstem areas that control eye movements. SNpr is GABAergic and inhibitory to the VLm (medial part of the ventrolateral thalamus) and VAmc (magnocellular part of the ventral anterior thalamus). 242.A. The dorsal lateral sulcus receives the dorsal roots. 243.D. The scan shows a diffusely enhancing brainstem glioma. Biopsy is usually not recommended in this case. Hyperfractionated radiation therapy has been shown to improve survival. Brainstem glioma represent 10 to 20% of childhood CNS tumors. There are currently no proven chemotherapeutic regimens. 245.C. 246.B. 247.B. 248.B. Lhermitte-Duclos disease is an uncommon cerebellar dysplasia that is characterized by hypertrophy of granular-cell neurons, and axonal hypermyelination in the molecular layer. Also known as dysplastic gangliocytoma of the cerebellum, it may occur in the setting of Cowden disease caused by a PTEN germline mutation. 249.A. There is no sensory deficit and no decrease in corneal reflex. There are no other symptoms in the other cranial nerves. 250.B. The liquid embolic agent n-butylcyanoacrylate is used in interventional neuroradiology. The embolic agents that are particulate in nature include polyvinyl alcohol (PVA), platinum coils, and silk thread. 251.C. The GCS in this case would be 13. Eye open to speech (3), the patient is confused (4), and he obeys motor commands (6). 252.B. The ciliospinal center of Budge is found in the lateral horn at T1. This is a sympathetic nucleus that innervates the radial muscle of the iris (dilator pupillae) and the nonstriated superior and inferior (Müller) muscles. 253.E. Aspirin decreases all anticonvulsant levels. 254.A. Posterior inferior cerebellar artery (PICA) syndrome causes decreased contralateral pain and temperature of the body. 255.C. Teardrop fractures occur when a fracture occurs on the anteroinferior edge of the vertebral body. The injury is due to hyperflexion and is unstable. Teardrop fractures are associated with anterior cord syndrome. 256.A. ITP is immune mediated, not related to an exogenous cause, and treatment of ITP is with steroids and splenectomy. TTP is nonimmune mediated and most often occurs in young females. 257.B. Dura and blood vessels are formed from mesoderm. 258.C. The most common primary septal tumor is astrocytoma. 259.C. The superior cerebellar artery is the most commonly conflicting artery in trigeminal neuralgia. 261.B. This MRI demonstrates a unilateral jumped facet with rotation in the cervical cord, compromising the spinal canal. 262.D. This particular AVM is best graded 4A. Its medium size (2), eloquent location (1), and deep drainage (1) place it as a Spetzler-Martin grade 4. The fact that it has stenotic venous drainage gives it a subclassification of 4A. 263.B. Biot (irregular) breathing is caused by a lesion in the dorsomedial medulla. 264.B. The anterior choroidal artery supplies the internal globus pallidus, posterior limb of the internal capsule, and temporal horn of the choroid plexus. 265.D. Pronator teres syndrome is different from carpal tunnel syndrome in that patients with pronator teres syndrome exhibit numbness in the palm and nocturnal exacerbations are rare. 266.C. Factor XIII deficiency exhibits normal bleeding parameters. 267.C. The area postrema is the only paired circumventricular organ. 268.B. Sweet and bitter tastes activate receptors coupled to G-proteins. 269.B. Although it is true that the pain starts at V2 (the lower side of the nose) and then involves V3 and V1, it is only necessary to treat the trigger zone. 270.E. Gerstmann’s syndrome is caused by a dominant parietal lobe lesion. Astereognosis is also caused by an anterior parietal lobe lesion, but is not part of Gerstmann’s syndrome. 271.E. Epidermoids of the skull show a lytic defect with a scalloped, sclerotic rim. They are slow growing and rarely show malignant transformation. 272.E. 273.B. Nightmares occur during REM sleep; night terrors may occur in either stage 3 or 4 sleep. Stage 4 sleep is associated with delta waves. 275.D. 276.B. A high-riding jugular bulb may be encountered during the drilling portion and should be tamponaded with hemostatic products and cottonoids. 277.B. The subcommissural organ is the only circumventricular organ with an intact BBB. 278.B. Dysgeusias are particularly prevalent in the elderly, and are often associated with the use of antihypertensives (e.g., captopril). 279.C. Gamma knife treatment is the best mode of therapy for an AVM that is smaller than 3 cm and located in an eloquent area. The angiogram shows a small subcortical right parietal AVM with a filling vessel arising from a branch of the right middle cerebral artery. Venous drainage is noted into the upper sagittal sinus. 280.D. Foster-Kennedy syndrome is usually caused from an olfactory groove or medial-third sphenoid wing tumor (usually meningioma). The classic triad is anosmia (ipsilateral), central scotoma (ipsilateral), and papilledema (contralateral). 281.B. Pick’s disease is characterized by severe focal atrophy commonly in the frontal and temporal lobes. This results in mental status and personality changes occurring in Pick’s disease patients. Pick bodies are positive for tau protein. 282.B. Fibrillation potentials are triphasic, last 1 to 5 milliseconds, and are caused by the activity of one fiber. 283.B. Sleep spindles (the burst described) and K complexes (sharp slow waves of high amplitude) are characteristic of stage 2 sleep. 284.D. This bony promontory seen in the picture is the posterior clinoid process and may be drilled carefully to expose the neck of the aneurysm. 285.D. The suprascapular nerve is trapped in the suprascapular notch. This nerve is the branch of the superior trunk. Atrophy of the supraspinatus and infraspinatus can result. 286.C. The abducens nerve crosses the medial lemniscus on exiting the brainstem. 287.B. The correct units are 50 mL/100 g/min. 288.D. 289.A. The most significant improvement noted postoperatively in the removal of frontal meningiomas involves attentional functions. There are no differences in memory, visuoconstructive abilities, or executive functions. 290.B. PML (progressive multifocal leukoencephalopathy) is caused by infection with group B human papovaviruses, principally JC virus. PML is typically bilateral, asymmetric, and most commonly involves the posterior centrum semiovale. 291.C. The substantia nigra pars reticulata neurons related to saccadic eye movements decrease their activity during the saccade. 292.D. 293.A. Research with model systems of seemingly disparate species (i.e., marine snail and the albino rat) suggest that neural mechanisms involved in associative learning may be highly conserved across species. 294.E. 295.C. Hypothermia is characterized by J-point elevation. 296.A. Anterior encephaloceles are compatible with normal intelligence in the majority of patients. Atretic encephaloceles also appear not to influence intellectual development and also have a lower incidence of hydrocephalus. 297.A. Giant cell glioblastoma is shown in the slide. The hallmark of giant cell glioblastoma is predominance on multinucleated giant cells and a high frequency of the TP53 mutation. 298.D. These features should not necessarily prompt the diagnosis of glioblastoma. 299.B. The supramarginal gyrus is at the posterior reach of the sylvian fissure. 300.A. Avellis’ syndrome is caused by a brainstem lesion that limits vagal innervation unilaterally, resulting in ipsilateral paralysis of the vocal cord and soft palate and loss of sensitivity to pain and temperature in the contralateral leg, trunk, arm, and neck. This syndrome is also called ambiguospinothalamic paralysis. 301.E. Bicuculline is a GABA-A antagonist. Muscimol is a GABA-A agonist. Kynurenate is a glutamate antagonist. Picrotoxin is a GABA inhibitor. 302.B. There is increased production of PMP22 in CMT disease. 303.C. Neurons in the spinal nucleus and in the ventral part of the chief sensory nucleus give rise to the crossed ventral trigeminothalamic tract. 304.D. In stroboscopic illumination at flicker rates below 15 Hz, the motion system is disabled. This explains why nightclub dancers are seen as moving discontinuously under a strobe light. 305.C. The tectospinal tract decussates in the dorsal tegmental decussation. Tectospinal fibers originate from deeper layers of the superior colliculus and distribute to cervical cord levels. Rubrospinal fibers decussate in the ventral tegmental decussation. 306.A. In the Royal Melbourne Hospital series of paranasal sinus cancers treated by craniofacial resection, sphenoid sinus involvement was the major predictor of later tumor recurrence. 307.E. Bipolar cells serve as interneurons between photoreceptor cells and ganglion cells. 308.D. 309.B. 310.C. The connatal form (type II) is clinically more severe and symptoms begin in the neonatal period. PMD results from mutations affecting the gene for proteolipid protein (PLP). 311.D. The pontocerebellar tract passes to the cerebellum via the middle cerebellar peduncle. The ventral spinocerebellar tract and the tectocerebellar tract pass through the superior cerebellar peduncle. 312.C. The lateral zone (dentate) send fibers to the VL thalamus and motor cortex (area 4). A lesion of the anterior lobe may cause slight hyperreflexia. 313.A. Dendrodendritic synapses have been found in the olfactory bulb and have been shown to be inhibitory; the granule cell processes make synaptic contacts with dendrites of mitral cells. Axodendritic synapses are excitatory. Axosomatic synapses are inhibitory and a classic example is the cerebellar basket cell contacting the Purkinje cell. 314.B. The parvocellular system of the dorsal lateral geniculate nucleus makes up ~80% of the total ganglion cell number. 316.E. These structures run in the floor of the body of the lateral ventricle. 317.A. The contents of the cubital fossa from medial to lateral are the median nerve, brachial artery, biceps brachii tendon, and the radial nerve. 318.D. The teres minor rotates the arm laterally. 319.C. The internal cerebral vein position can be confirmed by superimposing the angiogram of the medial posterior choroidal artery with the venous phase. The internal cerebral vein and the medial posterior choroidal artery occupy the same position when the arterial and venous phases are superimposed. Both of these structures course within the cistern of the velum interpositum. 320.B. 321.D. The Botzinger complex is the principal source of reciprocal inhibition in the respiratory network. It is composed of a cluster of cells at the rostral-most tip of the ventral respiratory group. 322.D. The posterior cord gives rise to the upper subscapular, lower subscapular, and thoracodorsal nerves. The latissimus dorsi is innervated by the thoracodorsal nerve. The subscapularis muscle is innervated by the upper and lower subscapular nerve. The teres major is innervated by the lower subscapular nerve. 323.A. The vast majority of children present with ischemic symptoms (TIAs, extremity weakness), whereas adults typically present with hemorrhage. 324.C. Valproic acid has a short half-life (~8 hours). Association with platelet dysfunction should alert the surgeon to the possibility of bleeding problems, especially in epilepsy cases. 325.B. Isoflurane allows patients to emerge from anesthesia faster and there is less hepatic effect from this agent. In addition, isoflurane produces the least increase in cerebral blood flow (CBF) of inhalational anesthetics. 326.C. The glomus is a prominent tuft of choroid plexus found in the atrium. 328.C. The premotor area plays a role in programming and sequencing learned complex movements. 329.E. 330.A. Theta activity has a frequency of 4 to 7 Hz. Other common EEG rhythms are delta (0–3 Hz), α (8–13 Hz), and β (>13 Hz). 331.B. The mesencephalic nucleus of the trigeminal nerve has pseudounipolar neurons. The mesencephalic nucleus extends from the pons to the upper midbrain. It receives input from muscle spindles and pressure receptors. 332.B. These second-order neurons give rise to axons that enter the cerebellum via the superior cerebellar peduncle. The ventral spinocerebellar tract conveys efference copies of motor commands for the lower extremities. 333.E. Narcolepsy is associated with HLA-DR2. HLA-B40 (children), HLA-B54 (adults), and HLA-A24 (both children and adults) are associated with moyamoya syndrome. HLA-B27 is associated with ankylosing spondylitis; of patients with ankylosing spondylitis, over 80% are HLA-B27 positive. However, this cannot be the only factor involved because only 2% of HLA-B27 positive individuals develop ankylosing spondylitis. 334.D. Awad et al. have demonstrated that the extent of mesiobasal resection determines the outcome after temporal lobectomy for intractable complex partial seizures. 335.E. Sydenham’s chorea is the most common cause of chorea. Also known as St. Vitus’ dance, this chorea occurs mainly in young females after a bout of rheumatic fever. 336.D. Decadron is shown in the picture. A postoperative course of an H2-receptor blocker is indicated for patients on glucocorticoid treatment. 337.D. 338.B. Vim stimulation is the procedure of choice when contralateral thalamotomy has been performed or is anticipated. 340.D. The H-reflex is a submaximal stimulation of mixed motor-sensory nerves, not enough to cause a direct motor response. The H-reflex is the electrical representation of the tendon reflex circuit. 341.B. The most common and pronounced aging effect on the brain is cell loss. 342.A. Stereognosis is an important function of the dorsal-column-medial lemniscal system. 343.C. Irrigation of fluid-coupled monitoring systems increases the infection rate nearly threefold. Thus irrigation should be performed infrequently and with exquisite sterile technique. 344.E. Area 4 fibers terminate in laminae VI–IX, whereas the postcentral gyrus fibers end mainly in laminae IV and V. The anterior corticospinal tract is an uncrossed tract in the (medial) ventral cord and terminates on lamina VII. 345.E. The paracentral lobule is supplied by branches from the anterior cerebral artery. 346.D. 347.D. 348.D. The sensorimotor GPi is located in the posterolateral part of the nucleus. 350.D. 351.C. Cowdry type A inclusions are intranuclear and are seen with cytomegalovirus (CMV), herpes, and subacute sclerosing panencephalitis (SSPE). Cowdry type B inclusions are intranuclear and are seen in acute poliovirus. The others listed are intracytoplasmic inclusions. Lafora bodies are seen in myoclonic epilepsy. Bunina bodies are seen in amyotrophic lateral sclerosis (ALS). 352.D. The dorsal spinocerebellar is an uncrossed tract. 353.D. Nystagmus in Meniere’s disease is horizontal and contralateral to the affected side. Past-pointing and falling occur toward the affected side. 354.A. The pulvinar has reciprocal connections with the inferior parietal lobule. 355.E. 356.B. Pineal tumors usually lie between the precentral cerebellar vein and the vein of Galen. The precentral cerebellar vein is usually displaced posterosuperiorly. This vein may be sacrificed if necessary. 357.C. The pharyngeal tubercle is found in line with the vomer and foramen magnum at the cranial base. 358.D. The anterior choroidal and lateral posterior choroidal supply the lateral ventricle. The medial posterior choroidal supplies the choroid plexus of the third ventricle. The posterior inferior cerebellar artery (PICA) supplies the choroid plexus of the fourth ventricle. 359.A. The final common pathway for platelet aggregation involves the binding of fibrinogen to the activated glycoprotein IIb/IIIa receptor on the platelet membrane. 360.D. Wilson’s disease (hepatolenticular degeneration) is a familial metabolic disease transmitted as an autosomal recessive trait. The abnormal gene has been assigned to the esterase D locus on chromosome 13. 361.B. Bergmann glia have cell bodies located in the Purkinje layer of the cerebellar cortex. 362.E. This is a lower motor neuron lesion and Babinski’s sign would not be expected. 363.C. The static labyrinth consists of the utricle and saccule. The vestibule is a central cavity of the inner ear that contains the saccule and utricle. 364.D. The ventral posteromedial (VPM) nucleus receives taste input via the ipsilateral central tegmental tract. The VPM nucleus receives sensory input from the head and oral cavity. 365.A. The lateral suboccipital retrosigmoid approach is best used for lateral tentorial notch meningiomas that extend infratentorially. 366.A. Calcifications are likely to be abnormal if encountered in children younger than 6 years. The incidence of pineal calcification is at most 40% by the age of 18. 367.E. The anterior longitudinal ligament attaches to the anterior tubercle of the atlas. The transverse ligament of the atlas is posterior to the dens. The apical and alar ligaments attach the dens to the foramen magnum. 368.B. The most frequent site of subependymoma is the fourth ventricle (50–60% of cases), followed by the lateral ventricles (30–40%). Less common sites are the third ventricle and septum pellucidum. 369.A. The lamina terminalis fills the interval between the anterior commissure and the optic chiasm. 370.A. Damage to the right frontal eye field (area 8) results in deviation of the eyes to the right. 371.D. Choroid plexus papillomas frequently display immunopositivity for transthyretin (prealbumin) and S-100. 372.B. Between 15 and 20 mL/100 g/min cortical evoked responses are lost and the EEG becomes isoelectric, but the neurons remain viable and are described as “idling.” At ~30 mL/100 g/min, the patient loses consciousness. 373.C. The lateral vestibulospinal tract is an uncrossed tract. 374.E. Lesions of the mediodorsal nucleus are found in patients with the Korsakoff amnestic state. 375.B. The trochlear nerve should be identified before transecting the tentorium. 376.C. Germinomas commonly occur in males in the first three decades. 377.D. Pathologically, CNS sarcoid is characterized by noncaseating granulomas. 378.A. Although other tumors may be more common after 1 year of life, choroid plexus tumors are the most common tumor in the first year of life. 379.B. “Square” ACA shift is usually caused by a holotemporal mass. 380.D. 381.A. The obex is the caudal apex of the rhomboid fossa and marks the beginning of the “open medulla.” 382.B. Hyponatremia (Na <130) can occur in up to 30% of ruptured anterior communicating artery aneurysms due to the local proximity of key perforators that supply the anterior hypothalamic nuclei. 383.C. 384.E. The optic disk (optic papilla) is located 3.5 mm nasal to the fovea centralis. It contains unmyelinated axons from the ganglion cell layer of the retina. The optic disk is the blind spot (contains neither rods nor cones). 386.C. 387.C. Plain film calcification is rarely seen. Calcospheres are also known as psammoma bodies. 388.E. The infraspinatus is innervated by the suprascapular nerve, which originates from the upper trunk of the brachial plexus. The subscapularis is innervated by the upper and lower subscapular nerves. The teres major is innervated by the lower subscapular nerve. The latissimus dorsi is innervated by the thoracodorsal nerve. The teres minor is innervated by the axillary nerve. 389.C. The time of development of effects of radiation is dose independent. 390.E. 391.E. Amplification of epidermal growth factor (EGF) occurs in glioblastoma. Double minutes (cytogenetic evidence of gene amplification) of N-myc occurs in medulloblastoma. 392.A. The Goldman cardiovascular risk score for noncardiac surgery indicates that a recent MI is a contraindication to elective surgery. 393.C. The fastigiovestibular tract is an efferent pathway that passes through the superior cerebellar peduncle (SCP) (uncinate fasciculus of the SCP). The juxtarestiform body is a component of the inferior cerebellar peduncle and contains afferent (vestibulocerebellar) and efferent (cerebellovestibular) fibers. 394.B. Bilateral destruction of both cunei results in a lower altitudinal hemianopia. 395.E. A posterior communicating artery aneurysm is prone to rupture with retraction on the temporal lobe. 396.B. Wave 5 is an indication of auditory nerve activity central to the tumor. It is easier to detect than the other waves. Wave 5 is generated in the brainstem. When used with N1 (monitors action potential of the auditory nerve), it is useful for predicting postoperative hearing function. 397.D. The most common symptom at initial presentation is referable to sensation. 399.C. Lars Leksell is called the father of modern day radiosurgery. 400.E. Broca’s aphasia results from damage to Brodmann area 44 (inferior frontal gyrus). 401.B. Canavan’s disease is associated with a point mutation of aspartoacyclase leading to elevated levels of NAA. 402.C. 403.A. Poxvirus is a DNA virus. Viral meningitis occurs in up to 50% of paramyxovirus infections (mumps). Rabies (rhabdovirus) targets the limbic tissue. DNA viruses cause SSPE, PML (papovavirus), and herpes encephalitis. RNA viruses are implicated in meningitis and AIDS. Herpes simplex encephalitis is the only CNS viral infection whose course and outcome are improved by specific antiviral therapy (acyclovir). 404.D. Hematoporphyrin derivative is an agent that is capable of photosensitizing malignant tumor cells. Other photosensitizers include rhodamine, acridine orange, phthalocyanines, and pyrilium derivatives. 405.B. The most sensitive cranial nerve to radiation is the optic nerve and the chiasm, with a single fraction dose tolerance of 8 Gy. 407.B. 408.D. Cerebellar glomeruli are synaptic connections that contain axons of incoming mossy fibers, axons and dendrites of Golgi type II cells, and dendrites of granule cells. Purkinje cells are not part of the glomerulus. 409.E. Focal white matter necrosis is the most common histologic evidence of radiation-related CNS injury. 410.D. 411.B. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) leads to subcortical ischemic damage, myelin loss, lacunar infarcts, and gliosis. 412.C. Exacerbation of peptic ulcer is the most common side effect of high-dose dexamethasone. 414.E. Because over 85% of CSF leaks from basilar skull fractures resolve spontaneously, the primary approach is expectant observation. Prophylactic antibiotics have not been shown to decrease the risk of meningitis and are not recommended. 415.C. A pituitary tumor that secretes thyroid-stimulating hormone (TSH) also frequently co-secretes the glycoprotein hormone α-subunit. An α-subunit/TSH ratio of >1 favors the diagnosis of TSH-secreting adenoma. 416.A. The superior (anterior) semicircular canal is identified by the arcuate eminence at the base of the skull. 417.D. The inferior orbital fissure is formed by the orbital surface of the greater wing of the sphenoid and the orbital surface of the maxilla. 418.A. Many spinocerebellar fibers are distributed to the medial vermal region of the anterior lobe of the cerebellum. 419.E. Aneurysms are not indications for radiosurgery. 420.C. The lesion is an epidermoid of the cerebellopontine angle. Epidermoids usually present in 20- to 40-year-olds. Unlike dermoids, they are not associated with midline defect. Spilling of their contents may cause a chemical meningitis or ventriculitis and therefore one needs to avoid spillage of tumor contents in the subarachnoid space. The main goal of therapy is complete excision of the tumor wall and contents to prevent recurrences. Radiation or chemotherapy has no role in the management. Steroids have been shown to be effective in preventing the inflammatory response and possible ventriculitis associated with these tumors. 421.B. Adrenoleukodystrophy displays X-linked recessive inheritance. 422.D. In cerebral salt wasting syndrome, there is inappropriate natriuresis and diuresis. 424.D. The fracture that initiates the leptomeningeal cyst may not be clinically evident, but most commonly involves the parietal bone. 425.C. Octreotide is fairly well tolerated; however, gallstone formation can develop in 10 to 20% of patients and is related to the inhibitory effect of octreotide on gallbladder motility. 426.D. 427.A. 428.E. The fetal Pcom is the most frequent of the persistent fetal circulations. 429.D. Angiography has no role in the management of acoustic tumor. 430.D. Interruption of Meyer’s loop fibers in the temporal lobe results in the “pie in the sky” lesion. 431.C. 432.C. 433.A. If a motor task is performed repeatedly to mastery, there is progressive attenuation of the cerebellar and premotor areas, with no change of activity of the primary motor cortex. 434.B. The classic lucid interval is only seen in one third of patients. Traction on the greater superficial petrosal nerve may occur with traction on the floor of the middle fossa. This may result in a dry eye postoperatively. 435.D. All are indications for craniotomy. 436.C. An ABI (auditory brainstem implant) is designed to stimulate auditory neurons of the cochlear nucleus and is placed in the lateral recess of the fourth ventricle at the time of acoustic tumor removal. 437.A. 439.E. Gyrus rectus may be removed (medial to olfactory nerve) to gain better visualization before clipping of an anterior communicating artery aneurysm. 440.C. At the optic strut, the ophthalmic artery pierces the dura to enter the orbit. After the origin of the ophthalmic, the internal carotid artery (ICA) passes the tip of the anterior clinoid process. 441.D. 442.B. The size of the hematoma is inversely related to the chance of the patient developing vasospasm. This reflects the fact that most of the blood has gone into the brain rather than the subarachnoid space. 443.A. Volatile anesthetics produce a dose-related reduction in CMR and a simultaneous increase in CBF. Intravenous anesthetic agents (except ketamine) decrease CMR and CBF in parallel. Volatile anesthetic agents increase CSF production. 444.E. The median sensory response, mediated by upper trunk fibers, would remain normal in lower trunk plexopathy. 445.D. An abnormal skin histamine response is a characteristic feature of patients with familial dysautonomia. 447.B. 448.B. 449.D. The lesion is a cavernous sinus meningioma. 450.C. The anterior inferior cerebellar artery loops around the cranial nerves VII and VIII. 451.D. The facial colliculus is located in the pontine half of the rhomboid fossa. The tuberculum cinereum (not to be confused with the “tuber cinereum” of the hypothalamus) is a surface eminence of the medulla that overlies the spinal trigeminal tract and nucleus. 452.C. Hemosiderin-laden macrophages are always seen with cavernous malformation. 453.C. Calcium channel blocking agents can be expected to have a beneficial effect in the patient; however, there is no effect on angiographic vasospasm and no increase in CBF. 454.D. The top of the cranial loop is the choroidal point, located in the telovelotonsillar segment of the PICA. The plexal point is the point where the anterior choroidal artery enters the choroidal fissure. 455.B. The principal anatomical substrate of perceptual organization is the posterior right hemisphere. Posterior right hemisphere disease tends to produce the most severe deficits of constructional praxis. 456.A. 457.B. 458.D. These tumors are rare, but must enter into the differential diagnosis of a solid third ventricle enhancing mass that is GFAP positive. 460.B. 461.E. 462.B. 463.A. 464.C. The recurrent artery of Heubner enters the anterior perforating substance and supplies the head of the caudate, anterior limb of the internal capsule, the anterior putamen and globus pallidus (GP), the septal nuclei, and the inferior frontal lobe. 465.C. The external sphincter is composed of circularly arranged striated muscle fibers that are mostly type I (slow twitch). 466.D. Harris’s method is the most clinically useful means of assessing atlantooccipital dislocation. The basion should lie within 12 mm of the superior continuation of a line drawn along the posterior cortex of the body of the axis; the distance of the basion and tip of the odontoid is normally less than 12 mm. 467.C. There are many more sodium channels located at the axon hillock. 468.B. Ganglioglioma is twice as common as DNET in causing temporal lobe epilepsy. 469.E. Huntington’s chorea is not an indication for radiosurgery. 470.E. There is a tendency for the posterior insula to drain more frequently into the deep system, whereas the anterior portion of the insula drains to the superficial venous system. 471.D. The primary fissure separates the anterior cerebellar lobe from the posterior cerebellar lobe. The horizontal fissure is located within the posterior lobe. The dorsolateral fissure is synonymous with the posterolateral fissure and separates the flocculonodular lobe from the posterior lobe. 472.E. Dural AV fistulas have a male predominance, are acquired lesions, have low flow, rarely hemorrhage, and have a gradual onset of symptoms. 473.B. Neurons in the penumbra (8 to 23 mL/100 g/min) survive but do not function. Below 8 mL/100 g/min neurons cannot recover. 475.D. Evidence for these areas influencing micturition comes from positron emission tomography (PET) scanning. 476.C. 477.C. 478.B. In a caudalis dorsal root entry zone (DREZ) operation, the electrode penetrates the dorsal spinocerebellar tract into the trigeminal tract and deeper caudalis nucleus. 479.C. The arterial dicrotic notch corresponds to the area between the tidal (P2) and dicrotic (P3) peaks of the ICP waveform. 480.A. The basal vein of Rosenthal receives tributaries from the medial temporal lobe and brain stem. It begins at the anterior perforated substance. 481.C. 482.D. Decussation of the superior cerebellar peduncles occurs in the caudal midbrain tegmentum at the level of the inferior colliculus. 483.B. Ascending pharyngeal artery supplies these nerves before anastomosing with vertebral artery branches. 484.B. Destruction of the abducent nucleus (subcortical center for lateral gaze) results in an ipsilateral lateral rectus and contralateral medial rectus palsy on attempted lateral gaze. 485.B. 486.D. The lateral subnucleus of CN III innervates the inferior rectus, inferior oblique, and the medial rectus. The medial subnucleus innervates the contralateral superior rectus. The central subnucleus innervates the levator palpebrae superioris. 487.C. 489.C. 490.D. The superior ophthalmic vein courses into the anterior cavernous sinus above the sixth nerve and below the first division of the trigeminal nerve. The superior ophthalmic vein is exterior to the annulus of Zinn. 491.E. The caudate nucleus forms the lateral wall of the frontal horn, body, and trigone of the lateral ventricle. It forms the roof of the temporal horn. The caudate does not extend to the occipital horn. 492.E. The dorsal trigeminothalamic tract is the rostral equivalent of the dorsal-column medial-lemniscal system. 493.D. The loose areolar tissue contains the valveless emissary veins. 494.A. Apocrine sweat glands of the axilla are innervated by adrenergic fibers, and secrete in response to mental stress. The eccrine sweat glands have cholinergic innervation. 495.B. The water content of the nucleus pulposus is maximum at birth and declines throughout life, the greatest decline occurring during the growth phase in childhood. 496.C. The tapeta are corpus callosum fibers connecting the temporal and occipital lobes. 497.D. 498.C. Cerebrospinal fluid is reabsorbed into the bloodstream through pressure-sensitive one-way valves in the arachnoid villi. 499.D. Pro opio melanocortin (POMC) gives rise to ACTH and beta-lipotropin. ACTH gives rise to α-MSH and CLIP. Beta-lipotropin gives rise to β-endorphin and gamma-lipotropin. 501.D. The ICA enters the cranium via the carotid canal of the temporal bone. 502.E. Damage to the trochlear nucleus results in damage to the contralateral superior oblique because the fibers decussate in the superior medullary velum. 503.A. The asterion is located at the intersection of the lambdoid, occipitomastoid, and parietomastoid sutures. This point reliably marks the anteroposterior level of the transverse-sigmoid sinus junction. 504.D. The anterior nucleus of the hypothalamus is involved in thermal regulation (dissipation of heat). The anterior nucleus stimulates the parasympathetic nervous system. Destruction of this nucleus results in hyperthermia. 505.D. Discs make up roughly 25% of the spine’s height. There is no disc at the occipitoatlantal joint, atlantoaxial joint, sacrum, or coccyx. 506.C. SIADH is a type of hyponatremia characterized by euvolemia. 507.D. Duane’s syndrome produces a characteristic pattern of eye movement with failure of abduction and retraction of the globe on adduction; the third nerve innervates the lateral rectus due to developmental failure of motoneurons in the sixth nerve nucleus. 508.C. Dilantin levels are decreased by carbamazepine. 509.A. Olivocerebellar fibers end as climbing fibers and aspartate is a common neurotransmitter in this connection. Reticulocerebellar and pontocerebellar fibers end as mossy fibers. 510.A. Tumor location is often more relevant than histology and other factors in assessing the prognosis of paraganglioma patients. For example, the metastatic rate of paraaortic paraganglioma is high (~30%), whereas that of carotid body tumors is much lower (~6%). 511.B. The anteromedial triangle can be used to expose the sphenoid sinus area. 512.B. Hyperperfusion encephalopathy is believed to result from the failure of intracranial vessels to compensate adequately for rapid increases of blood pressure. The posterior brain regions exhibit reversible edema bilaterally. 513.A. 514.C. The posterior circulation has sparse sympathetic innervation and is less well protected from hyperperfusion encephalopathies. 515.D. The central sulcus rarely joins the lateral sulcus. 516.B. Ipsilateral flushing is seen with cluster headaches. Cluster headaches also have an increased intraocular pressure, increased local skin temperature, male predominance, and are seen in older patients. 517.E. The syndrome described is Balint’s syndrome. It is of interest to note that functional “streams” of visual processing have been postulated. The “where” stream is destined for further processing in the parietal lobes and subserves spatial localization and the control of eye movements. The “what” stream is destined for the temporal lobes and is concerned with the identification of objects and color vision. Evidence for this came from studying patients with Balint’s syndrome. 519.A. 520.D. The gluteus minimus is a medial rotator of the thigh. The others listed are all lateral rotators. 521.C. Lewy bodies are concentrically laminated, round bodies found in vacuoles in the cytoplasm. They are absent in MSA. 522.B. 523.B. Paresthesias of the fingertips or mouth indicate that the electrode is too posterior (in the region of the VC). The electrode needs to be repositioned more anteriorly. High-frequency stimulation of the VC causes contralateral pares-thesias. The threshold for inducing contralateral paresthesias is higher in Vim (target) and it’s usually greater than 3 V. 524.C. Deficiency of the late complement components predisposes to Neisseria meningitidis. 525.B. Meningiomas and choroid plexus papillomas are the most common neoplasms of the trigone of the lateral ventricle. Meningiomas originate from the arachnoid cap cells of the choroid plexus and the tela choroidea. 526.B. The status of systemic disease is the most important determinant. 527.B. Golgi tendon organs are associated with Ib (A-α) fibers. Muscle spindles are associated with Ia (A-α) fibers. Slow pain and temperature are carried by unmyelinated fibers IV (C). 529.D. There is a greater risk of shunt infection with proximal revisions. 530.B. The development of sarcomas after cranial irradiation is well described. Fibrosarcomas are the most common type arising in the sella after irradiation for pituitary tumors. 531.D. 532.D. The sequence of ADH hormone release after surgery is triphasic. Initially, excessive diuresis is due to disruption of the pituitary stalk. Then, there is a release of ADH in large amounts from degeneration of distal axons. Finally, the stored ADH disappears and excessive diuresis returns. 533.E. Patients with infection commonly present with cord compression due to the predilection of echinococcus for bone, particularly vertebrae. 534.B. The mediodorsal nucleus is reciprocally connected to the prefrontal cortex. 535.C. Lymphoma metastatic to the brain tends to localize to the meninges, as opposed to the intraparenchymal (often subependymal) location of primary tumors. 536.C. The hippocampal commissure is located in the posterior component of the forniceal structure. 537.E. The centromedian nucleus is reciprocally connected to the motor cortex (area 4). 538.B. During surgery around the mastoid process, care must be taken to avoid injury to cranial nerve VII as it exits through the stylomastoid foramen, which is located medial to the insertion of the posterior belly of the digastric muscle at the digastric groove. 539.D. In addition, postoperative amnesia may result from manipulation of the fornix. 540.D. The rostral one third of the red nucleus receives dentate fibers, and the caudal two thirds receive fibers from the interposed nuclei. Stimulation of the red nucleus elicits increased tone in the contralateral flexors. 541.E. 542.E. Ketamine anesthesia increases CMRO2. All other anesthetic drugs decrease CMRO2. 543.D. The globus pallidus projects to three thalamic nuclei via the thalamic fasciculus is also known as Forel’s field H1 (FFH1). 544.D. The major blood supply to ventricular trigone meningiomas is constant, arising from the anterior choroidal artery with only a minor component arising from the posterior choroidal artery. 545.D. Elevated markers are indicative of malignant germ cell tumors and these tumors are radiosensitive and chemosensitive, precluding surgery. 546.A. 547.C. The GCS is 9. She opens eyes to pain (2), mumbles sounds (2), and the best motor response is localizing (5). Always take the best motor response when assessing GCS. 548.B Ewing’s sarcoma may present with involvement of the dura and skull, and or C. may extend to the underlying parenchyma. 549.E. This is a calvarial metastasis, an occurrence observed not uncommonly with metastatic breast carcinoma. 550.D. Sinonasal carcinoma may metastasize to multiple dural-based locations. 551.B. Recurrence after maximal radiation is an indication to operate. 552.B. 553.C. Diphtheria toxin has a predilection to sensory and motor nerves of the limbs and ciliary muscles or nerves. 554.A. Tetanus may typically present with trismus, risus sardonicus, tonic spasms, and generalized convulsions. 555.B. Symptoms appear 12 to 48 hours after ingestion and may be preceded by nausea, vomiting, and diarrhea. The convergence difficulty is usually followed by ptosis and extraocular muscles paralysis. 556.D. This is a typical feature of Reye’s syndrome. 557.C. Patients with spinal multiple myeloma typically present with hypercalcemia, bone pain characteristically absent at rest, and spinal canal invasion in ~10% of cases. 558.B. Myeloma cells in two or more peripheral blood smears are required. 559.C. It represents spread via spinal epidural veins. 560.C. Facioscapulohumeral dystrophy, or Landouzy-Dejerine’s syndrome, is associated with a defect on chromosome 4. 561.A. Werdnig-Hoffman’s disease has autosomal-recessive inheritance on chromosome 5q. 562.E. Myotonic muscular dystrophy has autosomal-dominant inheritance on chromosome 19. 563.B. Cri-du-chat is due to a 5p deletion and results in microcephaly, hypertelorism, and congenital heart disease. 564.D. Friedreich’s ataxia has autosomal-recessive inheritance on chromosome 9. 565.B. Diltiazem is the preferred agent for patients with systolic heart failure as it produces less myocardial depression than verapamil. 566.A. Verapamil’s side effects include hypotension and worsening of systolic heart failure due to negative inotropic effect. 567.C. Digoxin is indicated for chronic rate control of atrial fibrillation. Because of its delayed action, however, it is not indicated in acute atrial fibrillation. 568.D. Procainamide is contraindicated in patients with prolonged Q-T interval as it prolongs Q-T interval and may be proarrhythmic. Its use is to convert atrial fibrillation to normal sinus rhythm. 569.E. Beta-blockers are indicated for rate control of atrial fibrillation in the setting of a hyperadrenergic state, such as acute myocardial infarction after bypass surgery. 570.B. Gliosarcoma has the same histologic features as glioblastoma multiforme. In addition, it does stain for reticulin (sarcomatous part of the tumor). 571.D. Blunt trauma injuries to the cervical vertebral artery are more often managed by ligation than repair. Ligation may be risky because ~20% of the general population has a complete collateral circulation. Proximal occlusion may be accomplished by an anterior approach with mobilization of the sternocleidomastoid. Endovascular treatment with detachable balloons is a valid option for management. 572.C. Arsenic causes peripheral neuropathy, nausea, and vomiting. 573.E. Lead causes encephalitis in children, also pica, irritability, seizures, abdominal cramping, ataxia, coma, and high intracranial pressure. 574.B. Manganese causes a Parkinson-like syndrome. 575.E. 576.A. Mercury causes peripheral neuropathy, cerebellar signs, psychologic dysfunctions, tremor, movement disorders, and renal tubular necrosis. 577.D. Aluminum may present with a picture of Alzheimer’s disease. 579.E. Uremia is most likely to cause potassium depletion. 580.B. Tetany is the first sign of magnesium depletion. Delirium occurs usually before convulsions. Increase in deep tendon reflexes is observed usually. 581.D. Ca2+ concentration is 3 mEq/L 582.B. The MRI scan demonstrates an intramedullary astrocytoma, which occurs most commonly in the cervical spine. Lower motor signs may be at the level of the lesion and may aid in localization. These types of tumors are the most common intramedullary tumors in children and are usually of fibrillary type. 583.C. 584.A. 585.D. 586.C. Rickets presents with increased alkaline phosphatase, decreased serum calcium and phosphate levels. 587.D. Paget’s presents usually with increased alkaline phosphatase, normal serum calcium and phosphate levels; serum calcium levels may be increased depending on the stage of the disease. 588.A. Hyperparathyroidism presents usually with increased alkaline phosphatase increased serum calcium and decreased or normal phosphate levels. 589.D. Primary osteoporosis presents usually with increased alkaline phosphatase normal serum calcium and phosphate levels. 590.B. Hypoparathyroidism presents usually with normal alkaline phosphatase decreased serum calcium and increased phosphate levels. 591.E. 592.B. 593.C. 594.A. 595.D. 596.C. Scan 1 shows a wedge infarct and scan 2 shows a typical watershed infarct 597.B. that can also be due to small embolic infarcts. Both endocarditis and occlu- 598.A. sive disease of a single artery may result in scan 1. Watershed infarcts may typically present with “man-in-a-barrel syndrome.” 599.B. 600.C. All the other choices result in an efferent defect. 601.D. Metabolic neuropathy is typically symmetric and bilateral and will rarely present with an afferent pupillary defect clinically. 602.C. An improvement in mixed venous oxygen content will often improve the hypoxemia in the setting of a shunt. 603.B. The half-life is 72 hours. 604.A. Conversion of prothrombin to thrombin is the most time consuming and is usually measured as the prothrombin time (PT); it is in the range of 11 to 13 seconds. 605.B. Image 2 shows a venous angioma, which can be caused be arrested development. 606.D. Dural arteriovenous malformation are usually acquired after dural thrombosis. Neither cavernous malformation (Image 1) nor venous angioma (Image 2) is an acquired lesion. 607.B. Blue rubber nevus syndrome is associated with venous angiomas. 608.D. 609.C. 610.E. 611.B. 612.A. 613.B. The glomerulus is formed by the Golgi cell, the granule cell, and the mossy fiber. 614.A. The granule cell is the only excitatory cell within the cerebellum. 615.D. Basket cells end in a rete of terminals around the Purkinje cell. 616.C. Purkinje cells synapse with the deep cerebellar nuclei. 617.D. Early signs of cyanide poisoning include general weakness, malaise, early giddiness, inebriation, confusion, headache, vertigo, dizziness, confusion, and hallucinations. Tachypnea and hyperpnea generally precede apnea. 618.E. All are important in wound healing. 619.D. Aminoglycosides act by inhibiting protein synthesis through irreversible ribosomal attachment. 620.D. Polymyxin does not cause neuromuscular blockade. 622.B. When removing an intramedullary spinal cord tumor, one is more likely to encounter dilated veins at the caudal end of the mass. The other points are general principles of spinal cord tumor resection. Note that it is useful to seek out the blood supply of the tumor before debulking to keep the field relatively free of blood. 623.A. Galactocerebroside accumulates in Krabbe’s disease. Ganglioside accumulates in Tay-Sachs and Sandhoff’s diseases. Long chain fatty acids accumulate in adrenoleukodystrophy. 624.C. The T-reflex represents the monosynaptic stretch reflex elicited by tapping a tendon. 625.C. The trochlear nerve arises at the level of the lower midbrain (inferior colliculus level). 626.D. The patient likely has Eaton-Lambert syndrome with oat cell carcinoma. 627.B. Total body potassium excess of 100 to 200 mEq is required to produce a rise of 1 mEq/L in serum potassium. 628.B. The ulnar nerve has no supply from the C6 root. 629.B. Cervical roots C2 and C3 innervate this muscle. 630.D. Involved in the phrenic nerve and the brachial plexus. 631.C. 632.D. Innervated by C3, C4 and C5 (dorsal scapular nerve). 633.E. Innervated by the pudendal nerve (S2–4). 634.B. Innervated by the accessory nerve and C2 roots. 635.A. Hypnagogic hallucinations are seen with narcolepsy. Hypnagogic or hypnopompic hallucinations are visual, tactile, auditory, or other sensory events, usually brief but occasionally prolonged, that occur at the transition from wakefulness to sleep (hypnagogic) or from sleep to wakefulness (hypnopompic). 636.E. Vitamin A intoxication is associated with pseudotumor cerebri. 637.A. Beriberi is associated with thiamine deficiency. 638.C. Increased serum homocysteine and methylmalonic acid is associated with vitamin B12 deficiency. 639.B. Pyridoxine deficiency is associated with lower extremity paresthesias. 640.A. Barbiturates are used as antiepileptics and in the treatment of intractable increased intracranial pressure. 641.C. Both picrotoxin and bicuculine are GABA receptor blockers. 642.B. Baclofen in used as a centrally acting muscle relaxant. 643.C. Bicuculline is a selective GABA antagonist directly at the site where GABA binds. 644.E. The two aneurysms are a calcified thrombotic basilar artery aneurysm and a posterior communicating artery aneurysm. 645.D. The lesion presented is a colloid cyst of the third ventricle. A lumbar puncture is contraindicated prior to the placement of a shunt or a ventricular catheter due to the risk of herniation. 646.D. Torsades de pointes presents with prolonged QT intervals. 647.C. In early ARDS, the chest x-ray may be unrevealing while the patient may present with a hypoxemia refractory to supplemental oxygen. 648.B. Bicarbonate therapy does not improve outcome in diabetic ketoacidosis, regardless of the severity of the acidosis. 649.B. The MRI shows an enhancing mural nodule with an associated cyst. Pathology shows highly vascular tissue and stromal cells characteristic of hemangioblastoma. 650.D. The following T2-weighted MRI shows enhancement of the medial temporal lobe, a finding representative of herpes encephalitis. 651.B. The superficial peroneal nerve innervates the peroneus longus and brevis, which evert the foot. A lesion of the deep peroneal nerve affects ankle dorsiflexion. A lesion of the common peroneal or sciatic nerve affects both ankle dorsiflexion and foot eversion. Sciatic nerve lesion also affects foot flexion and inversion. 652.C. The order of the brachial plexus structures is root, trunk, division, cord, branch. 654.D. Aberrations of genes coding for cell cycle regulatory proteins involved in the control of G1/S phase transition have been found in gliomas and include mutation or deletion of genes like p53, retinoblastoma, cyclic AMP-dependent kinase number 2 (CDKN2) A/B, and amplification or overexpression of CDK4 and CDK6. 655.B. Oligodendrogliomas may exhibit loss of chromosomal regions on 1p and 19q13. Other chromosomal regions that may be lost from oligoden-drogliomas are 1p36, 9p, and 22. There may be evidence of increased numbers of chromosome 7. 656.D. The superior hypogastric plexus lies in front of the promontory of the sacrum between the two common iliac arteries and is sometimes called the presacral nerve. It then divides into the right and left inferior hypogastric plexuses. 657.C. The Papez circuit includes the cingulate gyrus, hippocampus, mammillary 658.C. bodies, and anterior nucleus of the thalamus. The lateral parabrachial 659.B. nucleus of the amygdala receives inputs from the lateral olfactory tract, pyriform cortex, hypothalamus, paraventricular thalamus, and the solitary tract nucleus. The medial septal nucleus projects from the fimbria of the hippocampus. 660.D. AIDS is frequently associated with platelets disorders in the ICU. 661.D. This MRI shows a vein of Galen malformation, which is usually associated with macrocephaly and hydrocephalus. 662.A. This MRI demonstrates an epidural abscess, which more frequently occurs in the thoracolumbar region. 663.B. Urinary magnesium loss is most prominent with loop diuretics. 664.C. The superior salivatory nucleus sends axons via the nervus intermedius (VII) to the greater superficial petrosal nerve and then to the pterygopalatine ganglion. 665.D. The occulomotor nerve (III) carries parasympathetics from Edinger-Westphal’s nucleus to the ciliary ganglion. 666.A. Arnold’s nerve is a branch of the vagus nerve (X) supplying sensation to the dura of the posterior fossa. 667.E. The deep petrosal nerve carries sympathetic fibers from the internal carotid artery from the superior cervical ganglion. 669.B. Dobutamine is an adrenergic agent that does not cause peripheral vasoconstriction. 670.B. Thiocyanate is cleared by the kidneys and its accumulation with the use of nitroprusside may cause a toxic syndrome. 671.B. Single punched out lesion without sclerotic edges is typical. 672.B. Eosinophilic granuloma may be a monostotic form of Langerhans cell histiocytosis. 673.C. In Paget’s disease, one may observe body destruction (early) and sclerosis (late). 674.A. Albright’s syndrome is characterized by unilateral fibrous dysplasia, pigmented skin lesions, and precocious puberty. 675.D. Epidermoid has characteristic scalloped edges. 676.A. Pneumocystis carinii pneumonia is the most common cause of ICU admission in HIV-positive patients. It is usually treated with trimethoprim-sulfamethoxazole. Toxoplasma is the most common intracranial infection in HIV-positive patients. 677.C. There are nine cases of transmission for every 10,000 exposures. 678.C. The lesion most likely represents a lobulated arachnoid cyst. 679.D. 680.A. The Golgi has a function in possessing enzymes that are extremely important in sugar and lipid chemistry of the eukaryotic cell. 681.B. The endoplasmic reticulum is important in drug detoxification; for example, adding hydroxyl groups to a lipid soluble type compound makes it more water soluble and thus easier to remove from the body. 682.B. Glycogen formation and breakdown occurs in the endoplasmic reticulum; this is particularly important in the liver. Glycogen, a polymer of glucose-1-phosphate, represents a quick source for energy. 683.C. Both the Golgi membranes closest to the nucleus (forming face) and the endoplasmic reticulum have a lamellar or tube-like membranous system. The Golgi membranes away from the nucleus (maturing face) are much more like plasma or organelle membranes. 684.C. True melanin is made by tyrosinase. 686.D. Total parenteral nutrition has been known to cause hypercapnia due to excessive carbohydrates promoting carbon dioxide retention, impaired oxygenation due to fatty acid damage to pulmonary capillaries, and acalculous cholecystitis due to bile stasis secondary to absence of lipids in the proximal small bowel. 687.A. This scan shows a teratoma that is associated with elevation of CEA levels. 688.B. Paraneoplastic sensory neuropathy with Anti-Hu antibodies is associated with limbic encephalitis (as seen on this MRI), seizures, epilepsia partialis continua, cerebellar ataxia, autonomic instability, myelitis with patchy weakness, and brainstem encephalitis. 689.A. Tabes dorsalis presents 15 to 20 years after initial syphilitic infection and is characterized by dorsal root and posterior column involvement as seen on this myelin-stained cord section. 690.C. Massive pulmonary embolism can result in significant increased dead space 691.C. and respiratory acidosis; on the other hand, smaller pulmonary embolisms can present with hyperventilation and hence respiratory alkalosis. Liver cirrhosis may also cause hyperventilation. Aminoglycosides can cause respiratory acidosis. 692.B. 693.A. 694.B. Tractography is a procedure to demonstrate the neural tracts. It utilizes special techniques of magnetic resonance imaging (MRI) and computer postprocessing. Information about direction of flow is provided by tractography but not about connections between different structures in the brain. 695.A. The scan shows an atypical dermoid cyst. Dermoid cysts can contain fat, which gives them a high signal intensity on T1-weighted sequences. A congenital dermal sinus tract can be associated with a dermoid cyst. Choice B is associated with paraganglioma. Choice C is representative of Antoni A pattern in acoustic neuromas. 696.C. The MRI scan shows bilateral acoustic neuromas, pathognomonic of neurofibromatosis type 2. Intertriginous freckling is a feature of neurofibromatosis type 1. 698.C. Methylprednisolone is not recommended in the treatment of emergent Addisonian crisis. 699.D. All three medications have been shown to help in the treatment of SIADH, with variable side-effect patterns. 700.A. Plasma types B and O can be safely transfused in a patient with blood type B as both these plasma types do not contain antibodies against B type blood. 701.E. Neurogenic shock is characterized by dilatation of arterioles and venules and decreased peripheral vascular resistance. It also presents with warm, dry skin, bradycardia, and hypotension. 702.A. The urinary system is most commonly involved in patients with gram-negative septicemia, followed by the respiratory system. 703.C. Stool culture has a sensitivity of greater than 90% in diagnosing C. difficile enterocolitis. Both latex agglutination and tissue culture assay for cytotoxin have a sensitivity of around 70%. Stool microscopy is not used to diagnose this condition. 704.D. Halothane increases cerebral blood flow the most; it is followed by enflurane and isoflurane. 705.C. Thiopental decreases intracranial pressure; the other listed agents increase intracranial pressure. 706.A. Isoflurane has been shown to cause tachycardia transiently in children. 707.B. Enflurane increases systemic vascular resistance. Isoflurane decreases it. 708.C. Both NF1 and NF2 have autosomal-dominant patterns of inheritance. 709.D. Retinal hemangiomas are associated with von Hippel–Lindau syndrome. 710.A. Iris hamartoma or Lisch nodule is seen in NF1. 711.D. Neurofibromatosis type 5 is the segmental type. 712.E. The anterior clinoid process is most likely going to have to be drilled to gain access to the neck of this aneurysm. 713.C. The superior cerebellar artery is seen in neurovascular conflict with the trigeminal nerve. More proximally, though, the artery is seen near the tentorium, which is in very close relation to the trochlear nerve. 715.D. Papaverine inhibits antiparkinsonian effect of levodopa. Fluconazole 716.C. increases serum phenytoin and decreases warfarin metabolism. Thyroid 717.B. hormones enhance clotting factor catabolism. Meperidine may cause hyper- 718.C. tension, rigidity, and excitation when used with monoamine oxidase 719.A. inhibitors. 720.D. The other medications tend to further exacerbate the symptoms of malignant hyperthermia. 721.C. Colon carcinoma has a predilection to metastasize to the liver and other visceral organs. 722.B. The lateral, medial, and posterior cords carry their names in relation to the second and third segments of the axillary artery. 723.C. This type of spondylolisthesis is caused by a defect in the pars interarticularis, occurs in 90% of cases at L5-S1, is usually bilateral, and is more common in males. 724.D. The superior outer quadrantanopia is due to involvement of von Willebrand’s knee. 725.A. 726.A. 727.C. 728.B. Meyer’s loops are interrupted causing a homonymous superior quadrantanopia. 729.E. 730.B. Ulnar nerve entrapment can occur at the arcade of Struthers. 731.C. Extensor carpi ulnaris palsy may be due to a constriction at the arcade of Frohse. 732.A. The brachial artery, along with the median nerve, passes under Struthers’ ligament. 733.A. Reservoir sign, or intermittent large-volume CSF rhinorrhea, is a relatively uncommon occurrence in patients with sphenoid sinus encephaloceles. The leak of fluid is usually insidious. 734.B. Scoliosis occurs in 66%, whereas radicular pain occurs in 50% of patients. 736.D. All are valid mechanisms. 737.D. De Quervain’s syndrome is characterized by tenosynovitis of the abductor pollicis longus and extensor pollicis brevis muscles. The nerve conduction velocities are typically normal. 738.A. The roof of the fourth ventricle contains both the superior and inferior 739.B. medullary veli. The floor of the fourth ventricle is formed by the rhomboid 740.B. fossa, which contains the facial colliculus and hypoglossal trigone. 741.B. 742.C. The scan shows a cephalohematoma, which is treated with head wrapping and possibly needle aspiration. 743.B. The notochord induces the formation of the neural plate and neural tube. The neural tube regions give rise to the alar and the basal plates. The alar plate contains sensory/integrative nerve cell bodies of brain and spinal cord and gives rise to the dorsal horn. The basal plate contains motor neurons of brain and spinal cord and gives rise to the ventral horn. 744.C. Cheyne-Stokes respiration occur with diencephalon lesions. Central neuro- 745.D. genic hyperventilation occurs with midbrain lesions. Apneustic respiration 746.B. occurs with pontine lesions. Ataxic respiration occurs with medulla lesions. 747.A. 748.B. 749.A. The middle cerebellar peduncle contains only afferent fibers. 750.B. The angiogram demonstrates a primitive trigeminal artery. The persistent acoustic artery passes through the internal auditory meatus. 751.E. The overall rate of HIV transmission from a single percutaneous exposure to HIV-infected blood is of the order of 0.3%. Postexposure prophylaxis (PEP) has been shown in one study to reduce this rate by 80%. 752.D. Epidemiologic studies of health care workers exposed to hepatitis C virus (HCV) through a needlestick or other percutaneous injury have found that the incidence of infection averages 1.8% per injury. 753.D. The risk of acquiring hepatitis B from a needlestick when the source was hepatitis B antigen-positive ranges from approximately 2 to 40%, depending on the source’s level of viremia. 754.D. The scan shows straight sinus thrombosis. 755.A. Malignant hyperthermia has an autosomal-dominant inheritance pattern. It may be caused by halothane or succinylcholine. Body temperature increase is about 1YC every 5 minutes. It is treated with dantrolene and discontinuation of the anesthetic. 756.D. The scan shows a cavernous angioma occurring at the thalamocaudate recess. These lesions may be associated with venous angiomas. 757.A. Type 1 modic changes show decreased intensity on T1-weighted images and increased intensity on T2-weighted images. Type 2 modic changes show increased intensity on T1-weighted images and isointense signal intensity on T2-weighted images. Histopathology on type 1 change demonstrates disruption and fissuring of the end plates and vascularized fibrous tissue. On type 2 changes, yellow marrow replacement is seen. Type 1 changes may convert to type 2 after a few years. There appears to be a spectrum of vertebral body marrow changes associated with degenerative disk disease. 758.D. The lesion represents a syrinx at the level of the inferior cerebellar peduncle. The abducens nerve arises at a higher level and is less likely to be affected. The anterolateral system courses ventral to the lesion and may be affected. The vestibulocochlear nucleus is also located at this level. 759.A. Ketamine raises systemic arterial blood pressure but not necessarily the perfusion in hypovolemic states. In hypotensive states of short duration from endotoxin treatment, it improved the hemodynamics by augmenting the perfusion and the systemic pressure. 760.C. The scans show a typical intramedullary ependymoma with blockage of CSF flow, which is associated with Froin syndrome (clotting and xanthochromia in the CSF) and Queckenstedt’s sign, which is failure of jugular vein compression to increase CSF. The cervical type of intramedullary ependymoma is usually of cellular type, more frequent in women in their mid-40s. 761.B. The MRI set demonstrates basilar meningitis with a trapped fourth ventricle and foramina of Luschka, which occurs in sarcoidosis. Elevated angiotensin-converting enzyme levels are also a feature of this disease. 762.B. The proximal tubule plays a role in secreting organic acids and reabsorbing 763.A. Na+, water, glucose, bicarbonate, amino acids, and phosphate. The distal 764.B. tubule’s role involves secretion of H+ and K+ and reabsorption of Na+ and Cl. 765.C. The glomerular filtration rate is at its peak in young adulthood, at about 120 mL/min. 767.A. Central neurocytoma looks like oligodendroglioma histologically but is positive for synaptophysin on immunohistochemistry. 768.A. The parietal operculum is caudal to the inferior frontal gyrus. Directly inferior to the inferior frontal gyrus is the sylvian fissure. 769.C. Nitric oxide promotes the formation of cyclic guanosine monophosphate (cGMP). 770.D. Symptomatic 70 to 90% stenosis of the carotid on the angiogram carries a risk 771.B. of stroke of 26% over 2 years, or 13% per year. Asymptomatic 70 to 90% 772.C. stenosis of the carotid on the angiogram carries a risk of stroke of 11% over 5 years, or 2% per year. Post–carotid endarterectomy in preoperative symptomatic 70 to 90% stenosis of the carotid on the angiogram carries a risk of stroke of 9% over 2 years, or 4.5% per year. 773.A. All the other medications cause hyperkalemia. 774.C. Intracellular methemoglobin appears as hyperintense on T1 and hypointense on T2, and is usually present from 3 days to 2 weeks after a hemorrhage. Extracellular methemoglobin, which appears after 2 weeks, is hyperintense on T1 and T2. The images show hyperintensity on T1 and iso- to hypointen-sity on T2, consistent with intracellular methemoglobin toward the end of 2 weeks following the hemorrhage. 775.C. Ethanol has a molecular weight of 46 and is lethal at levels greater than 350 776.D. mg/dL (least lethal). Methanol has the lowest molecular weight (32) and is the least lethal out of the three remaining substances (need 80 mg/dL for lethality). Ethylene glycol has the highest molecular weight (61) and is the most lethal (only need 21 mg/dL to cause death). 777.E. Cryoprecipitate is used to treat acute blood loss in von Willebrand’s disease. 778.D. The scan shows a foramen magnum tumor. All the stated clinical findings are associated with this tumor location; however, neurogenic bladder tends to occur very late. 779.D. Autonomic symptoms occur early. 780.A. There is no sensory dissociation.
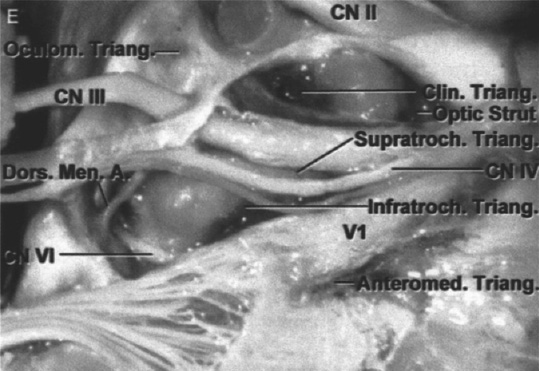
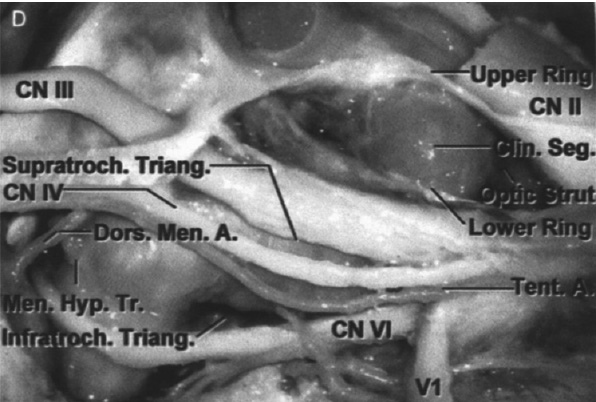
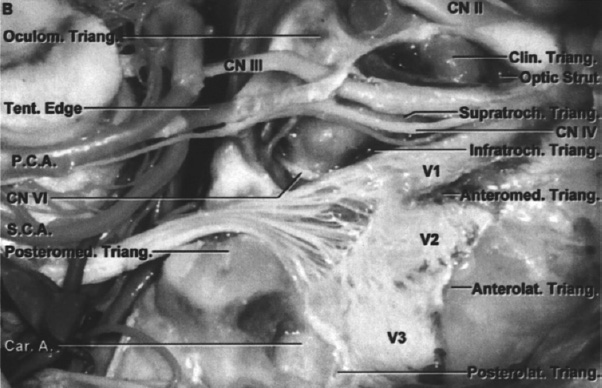
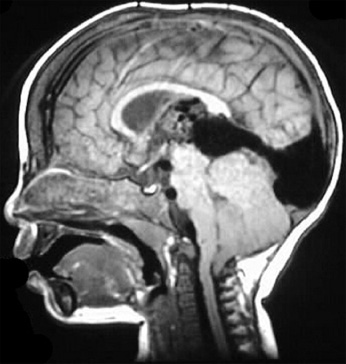
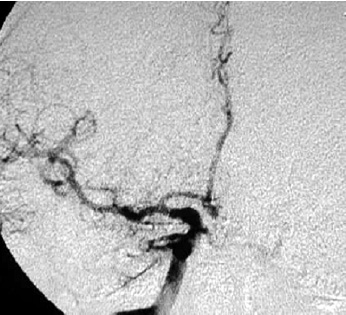
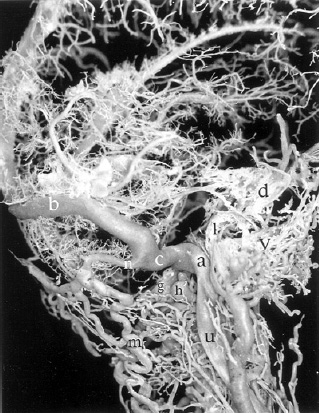
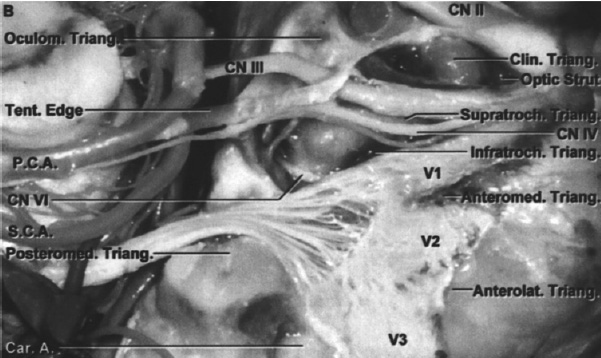
| Conus Medullaris Syndrome | Cauda Equina Syndrome | |
| Presentation | Sudden and bilateral | Gradual and unilateral |
| Reflexes | Knee jerks preserved but ankle jerks affected | Both ankle and knee jerks affected |
| Radicular pain | Less severe | More severe |
| Low back pain | More | Less |
| Sensory symptoms and signs | Numbness tends to be more localized to perianal area; symmetrical and bilateral; sensory dissociation occurs | Numbness tends to be more localized to saddle area; asymmetrical, may be unilateral; no sensory dissociation; loss of sensation in specific dermatomes in lower extremities with numbness and paresthesia; possible numbness in pubic area, including glans penis or clitoris |
| Motor strength | Typically symmetric, hyperreflexic distal paresis of lower limbs that is less marked; fasciculations may be present | Asymmetric areflexic paraplegia that is more marked; fasciculations rare; atrophy more common |
| Impotence | Frequent | Less frequent; erectile dysfunction that includes inability to have erection, inability to maintain erection, lack of sensation in pubic area (including glans penis or clitoris), and inability to ejaculate |
| Sphincter dysfunction | Urinary retention and atonic anal sphincter cause overflow urinary incontinence and fecal incontinence; tend to present early in course of disease | Urinary retention; tends to present late in course of disease |
782.B. With bilateral internuclear ophthalmoplegia, there is an adduction deficit in both eyes. This is observed in bilateral lesions on the medial longitudinal fasciculus.
783.A. Preganglionic sympathetic fibers secrete acetylcholine.
784.B. The locus ceruleus contains noradrenaline.
785.B. The periaqueductal gray contains the locus ceruleus. It also contains the dorsal raphe nucleus and enkephalin releasing neurons.
786.C. Both Wernicke’s and global aphasias display repetition and comprehension deficits.
787.C. Watershed infarcts occur in areas between the major vascular territories and are due to a global decrease in cerebral perfusion.
788.D. McConnell’s capsular arteries arise directly from the intracavernous carotid artery.
789.D. Radionuclide scans have a relatively high sensitivity in detecting discitis.
790.A. NAA, found in neurons and axons, is used as a neuronal marker. A reduction in the NAA signal reflects neuronal loss or injury, as seen in many brain
pathologies including neurodegenerative diseases. NAA peaks typically represent neuronal density. Moderately increased choline peaks and reduced NAA signal intensities indicate low-grade gliomas; high-grade tumors are characterized by distinctly higher choline peaks and even lower NAA signals. The presence of lipid signals indicates tissue necrosis.
791.B. Aspergillosis has a predilection for the basal ganglia in some cases. It tends
792.D. to invade blood vessels, cause hemorrhagic infarcts, and may cause formation of paranasal sinus mycetoma. Coccidioidomycosis can cause meningitis and caseating granulomas. The diagnosis of early cerebral infarction in a patient considered at risk for invasive aspergillosis even without overt pulmonary disease is an indication to institute aggressive antifungal therapy.
793.C. The MRI scan demonstrates leptomeningeal gliomatosis associated with a high-grade glioma in the left occipital area. The best therapeutic option, given the diffuse nature of the disease is, initially, chemotherapy and radiation.
794.C. The glossopharyngeal nerve innervates the stylopharyngeus.
795.D. Functional residual capacity (D) does not change during exercise, and is usu-
796.D. ally 2.4 L; it is the sum or residual volume (C) and expiratory reserve volume
797.B. (ERV), or the difference between vital capacity (B) and ERV. VC is usually
798.C. around 4.4 to 5 L and is measured by having the patient inhale profoundly and exhale fully into a spirometer. Residual volume cannot be measured directly and needs to be calculated as a percentage of exhaled versus inhaled 10% helium containing solution.
799.C.
800.B. Point 3 on the MR spectroscopy represents an area of tumor (glioma), which shows an elevated Chol/Cr ratio and a decreased NAA peak.
801.B. The formula represents oxygen uptake.
802.D. (Cc O2 − Ca O2 )/ (Cc O2 − Cv O2 ) = Qs/Qt = shunt fraction.
803.A. Q= Pπr4/8 VL.
804.C. If the pencil is pulled from his eye, there should be adequate measures to stop bleeding and irrigate the wound. This can only be done properly in the operating room. This patient should be managed with antiepileptic medication, broad-spectrum antibiotics, CT scan, immediate open surgical debridement, and follow-up MRI in a week.
805.D. The patient has ossification of posterior longitudinal ligament (OPLL), which is best managed with cervical corpectomy and fusion.
< div class='tao-gold-member'>
Related posts:
 Questions
Questions
 Answers
Answers
 Questions
Questions
 Temporal Gyrus Versus Inferior Temporal Gyrus Transcortical Approaches to High-Grade Astrocytomas in the Mediobasal Temporal Lobe: A Comparison of Outcomes, Functional Restoration, and Surgical Considerations
Temporal Gyrus Versus Inferior Temporal Gyrus Transcortical Approaches to High-Grade Astrocytomas in the Mediobasal Temporal Lobe: A Comparison of Outcomes, Functional Restoration, and Surgical Considerations
 Targeting Mechanisms of Typical Indications of Acupuncture
Targeting Mechanisms of Typical Indications of Acupuncture
 4 Imaging Techniques in Acute Ischemic Stroke
4 Imaging Techniques in Acute Ischemic Stroke



