Fig. 5.1
Standard anterior approach to the lumbar spine via midline laparotomy. The bowel has been rotated out of the peritoneal cavity and is protected on the patient’s abdominal wall with towels. The device at the lower left projecting from the patient’s anterior iliac region is a registration device for the frameless stereotactic navigation system. The need to protect vital structures such as bowel and blood vessels presents a major challenge in the development of true image guided percutaneous spinal fusion devices entering from a direct anterior approach
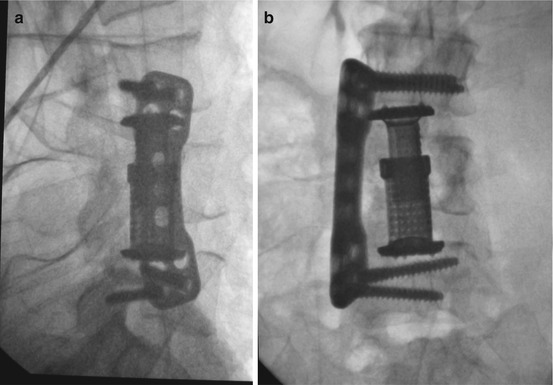
Fig. 5.2
L3-L5 stabilization via a right extracavitary retroperitoneal approach, anterior-posterior (a) and lateral (b) views. In this case, a leiomyosarcoma centered at the L4 vertebral body was resected, followed by application of a vertebral body replacement device and lateral buttress plate. While bowel and iliac vessel issues are largely avoided as compared to the direct anterior approach of Figure 1, the compromise is a more restricted field of view as well as the need to understand the location of the artery of Adamkiewicz
Until now, lateral interbody fusion has been considered a technique dependent exclusively on fluoroscopic guide: nevertheless, as for the most of fluoroscopic-guided procedures, this implies higher radiation dose exposure for both the physician and the patient. Recently however, a fully CT-guided lateral interbody fusion technique has been proposed, to reduce radiation exposure. Moreover, thanks to a CT-guided technique, the surgeon has the possibility to control bowels and muscle position, as well as vascular structures, to avoid complications related to accidental damage to these structures [2].
When the surgeon has to obtain interbody fusion, the conventional anterior approach to the L5–S1 disk space can be a real challenge, as abdominal bowels and vessels has to be exposed. By using CT-guided/fluoroscopic-guided technique, a novel minimal invasive percutaneous para-coccygeal approach to L5–S1 space can be adopted, providing an alternative route to the disk space and making possible both the discectomy and the interbody fusion with adequate tools [3].
The minimally invasive approach that is the nearest to a true anterior open approach is the lateral trans-psoas approach (“extreme lateral interbody fusion” or “XLIF”) (Fig. 5.3): this approach was proposed by Taylor and coworkers [4] and is now adopted not only in posttraumatic or degenerative disease but in case of adult degenerative scoliosis correction also, particularly at lumbar levels [5, 6].
Fig. 5.3
Multi-level lumbar anterior interbody fusions, L2-L3, L3-L4, and L4-L5, anterior-posterior (a) and lateral (b). The approach used in this case was direct lateral trans-psoas, which also allowed for the application of lateral buttress plates. Note on the axial image (c) that, unlike a posterior approach, an anterior approach allows for placement of an interbody cage with a large surface area “footprint” that extends from lateral edge to lateral edge of the vertebral body
This approach utilizes a retroperitoneal corridor, not so far away from the route conventionally used in more widespread procedures, that is developed with progressive coaxial dilators that allow to get the target with small singe cut and, finally, the placement of a long-bladed retractor system. The psoas muscle is traversed until the disk space is encountered. Visualization is necessarily limited to the lateral perspective if the procedure is performed on a fluoroscopic guide, but access to the most anterior surfaces of the vertebral body and disk space is still readily achieved. There are several recent papers describing the advantages of XLIF approach in comparison with the anterior one, as a smaller incision, surgical time and post-op pain reduction, as well as a more precise placement of the device, and indication has been extended not only to degenerative disease but to infection and tumor disease also [7].
When a CT-guided technique is performed, clearly depiction of psoas muscles makes easier the disk space approach. Since a direct lateral line of attack is in use, the iliac crest impedes if not prohibits this approach from being useful below L4–L5 [8, 9].
True percutaneous image-guided approaches to the anterior lumbar spine are in their infancy. Efforts are underway to merge navigation techniques, such as stereotaxy, with endoscopes containing working channels (Fig. 5.4). Barriers to such strategies include the need to deliver implants through small-diameter corridors and the protection and mobilization of intervening structures, such as the bowel. One promising avenue under development is an approach through Kambin’s triangle, which uses an oblique lateral trajectory similar to the approach angle for discography and disk space aspiration (Fig. 5.5) [10]. When a CT-guided technique is adopted as guidance of the treatment, the risk of complication can be definitely reduced.