Chapter 20 Anterior Approaches to the Cervicothoracic Junction
TRANSCLAVICULAR–TRANSMANUBRIAL APPROACH
Radiological studies of the upper thoracic spine have indicated that at least the T3 vertebra can be visualized in the majority of patients in whom a suprasternal approach is undertaken after the splitting and mobilization of the manubrium.1
The external landmarks for level identification are T2–3 at the suprasternal notch and T4–5 at the sternal angle (Fig. 20-1). Before adopting this approach, it is important preoperatively to confirm the extent of the lesion and the position of the upper margin of the sternum on lateral radiographs. It also is essential to assess the affected spinal cord level and its relation to the level of the upper margin of the sternal manubrium because this relationship varies among individuals.
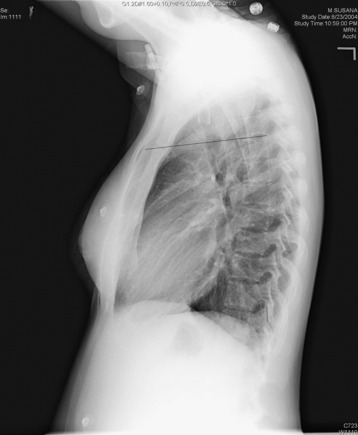
Fig. 20-1 In this patient, the sternomanubrial junction corresponds to the T2–3 intervertebral disc level.
BONE REMOVAL
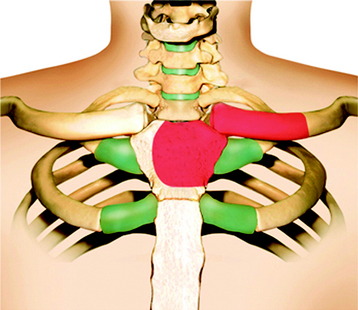
The medial third of the clavicle and manubrium is dissected periosteally. The clavicle is divided at the junction of the medial and middle thirds (Fig. 20-2). All procedures are safe when the periosteum is separated from the bone by using a raspatory. While excising the sternum, the sternum lining is carefully separated using the raspatory to avoid possible damage to the internal mammary artery (Fig. 20-3).2

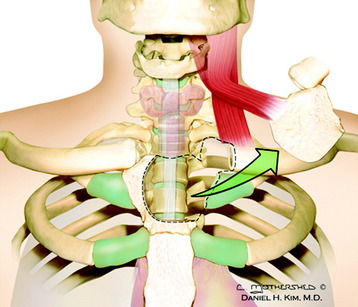
The left side of the manubrium can be removed piecemeal along its posterior periosteum.
Alternatively, the manubrium and sternoclavicular joint can be left intact and reflected with the sternal head of the sternocleidomastoid muscle (Fig. 20-4).
VASCULAR DISSECTION
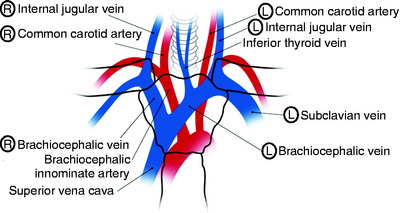
Dissection is carried deeper until the great vessels are identified. Inferior thyroid vessels can be ligated. If the cranial part, approximately 50% of the sternal manubrium, is removed, the surgeons do not need to retract the left innominate vein. A bilateral retraction of the brachiocephalic trunk can expose the T1 and T2 vertebral body (Fig. 20-5).
TRANS-STERNAL–TRANSTHORACIC APPROACH
SKIN INCISION AND CERVICAL DISSECTION
The supine position is set with the neck hyperextended. A linear vertical incision starts from the mid-cervical spine along the anterior border of the sternocleidomastoid muscle and continues through the middle of the sternum down to the tip of the xiphoid process (Fig. 20-6).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


