♦ Preoperative
Operative Planning
- Imaging
- Magnetic resonance imaging (MRI)
- Computed tomography (CT) myelogram if MRI is inconclusive
- Flexion/extension x-rays
- CT scan may be helpful/necessary to assess presence/configuration of os-teophyte and to better understand bone anatomy/quality
- Magnetic resonance imaging (MRI)
- Monitoring (e.g., motor evoked potentials, somatosensory evoked potentials, electromyography) may be considered depending on patient’s pathology, monitoring availability, and local/surgeon practice
Equipment
- Basic spine tray
- Additional helpful instruments:
- Small “pediatric” Weitlaner retractor (blunt ideal)
- Debaky forceps, vascular clips
- Kittner dissector sponges
- High-speed drill (Midas Rex with AM-8 bit; consider angled handpiece and diamond burr)
- Small “pediatric” Weitlaner retractor (blunt ideal)
- Anterior cervical retractor set (e.g., Shadow-Line [V Mueller Neuro], TrimLine [Medtronic], Thompson-Farley)
- One- and 2-mm Kerrison punches with thin footplates
Operating Room Set-up
- Headlight
- Loupes
- Microscope
- Bipolar cautery and insulated-tip Bovie cautery
- Intraoperative x-ray and/or fluoroscopy
Anesthetic Issues
- Some patients require special intubation techniques (fiberoptic, glide scope) to minimize neck manipulation (especially extension)
- Prophylactic intravenous antibiotics (cefazolin 2 g for adults) 30 minutes prior to incision. Consider vancomycin for instrumentation.
- Foley catheter for prolonged surgery
- Consider arterial line for patients who require enhanced monitoring of blood pressure
- Special anesthetic regimens may be needed if spinal neurophysiological monitoring used
- Bite block when using motor evoked potentials
- Foley catheter for prolonged surgery
♦ Intraoperative
Positioning
- Head on soft padded “doughnut” in neutral position (especially if fusion to be performed)
- Gentle cranial extension with shoulder roll (as tolerated)
- Appropriate padding to prevent pressure neuropathies
- Arms tucked at sides. Gentle shoulder traction may be helpful but use caution to avoid/limit brachial plexus stretch.
- Intraoperative x-ray/fluoroscopic imaging used to confirm cervical alignment and guide incision
Planning of Sterile Scrub and Prep
- Use disposable clippers for minimal shave (if needed)
- Betadine detergent scrub
- Alcohol wipe (avoid leaving residual as potentially flammable with intraoperative sparks from cautery)
- Sterile towel to dry
Mark Incision
- Localization using anatomic landmarks and intraoperative x-ray
- Transverse curvilinear incision in skin crease for most cases
- Consider longitudinal incision along medial sternocleidomastoid muscle for difficult anatomy or many levels
- Consider injection of subcutaneous lidocaine with epinephrine (may minimize skin bleeding and patient stress)
Exposure
- Incision with #10 or #15 blade
- Along incision line, elevate and divide platysma sharply with Metzenbaum scissors or Bovie cautery (with attention to underlying veins)
- Dissect along medial border of sternocleidomastoid
- For lower cervical approach, identify omohyoid (usually around C5–C6, may divide if needed but can usually work above it)
- Identify, protect, and work medially to the carotid sheath structures
- Kittner dissectors and handheld Cloward retractors helpful to identify/ develop appropriate plane to expose longus coli muscles, prevertebral fasica, and underlying disc spaces and vertebral bodies
- Verify levels with x-ray/fluoroscopy
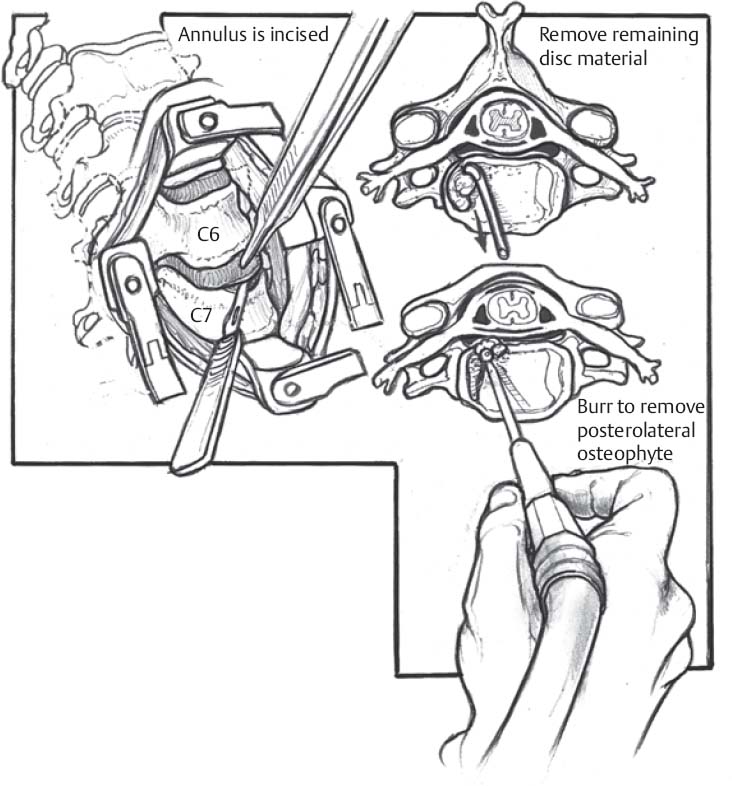
Discectomy/Decompression (Fig. 94.1)
- Insert self retaining anterior cervical retractor system (multiple options, see above for examples)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


