♦ Preoperative
Operative Planning
- Review patient’s history for bone metabolic disease, osteoporosis/osteopenia
- Review patient’s history for diabetes, smoking, and other factors that may affect fusion success rate and therefore intraoperative and postoperative management
- Review preoperative and/or intraoperative imaging to help determine dimensions of area to be instrumented
- Anticipated length of plate to be used
- Anticipated length of screws to be used based on size of vertebral body
- Anticipated length of plate to be used
Equipment
- Select anterior cervical plating system (multiple options of each type)
- Constrained plate systems
- Semiconstrained plate systems
- Dynamic plate systems
- Constrained plate systems
♦ Intraoperative (Fig. 98.1)
Positioning
- Maintain head in neutral position as head turn may lead to unintended fixation in rotated position
Exposure, Decompression, and Reconstruction
- As per primary procedure
- Remove/reduce anterior osteophytes
- Osteophyte rongeur
- Drill (caution to protect surrounding soft tissue structures to limit chances of injury if drill “kicks”)
- Osteophyte rongeur
- Helpful to know width of plate to be inserted
Plate Selection/Placement
- Measure length of area to be spanned by plate (top of superior graft to bottom of inferior graft)
- Use that length to direct plate selection
- Measure distance between bottom of top screw hole to top of bottom screw hole
- Use shortest plate than allows this dimension to allow plate to fully span graft(s)
- Measure distance between bottom of top screw hole to top of bottom screw hole
- Plate may need contouring to match surface of spine (e.g., degree of lordosis)
- If plate contoured, make sure to recheck measurements as length can change
- Carefully adjust retractors to place plate with direct vision and avoidance of soft tissue injury
- Consider use of temporary plate-holding pins
- Verify plate position with x-ray/fluoroscopy
Screw Selection/Placement
- Screw size based on local anatomy, preoperative imaging, and intraoperative imaging
- Most systems do not require bicortical purchase (although may still be
- Rostrocaudal screw angle (Figure 98.1)
- May be directed by plating system
- Should also reflect local anatomy and intraoperative imaging
< div class='tao-gold-member'>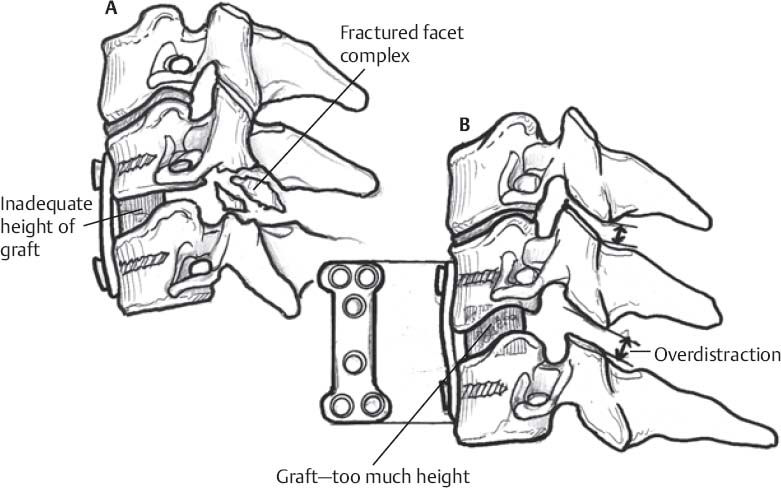
Fig 98.1 Schematic of (A) inadequate graft height with secondary facet fracture, and (B) graft overdistraction.
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel
- May be directed by plating system


Full access? Get Clinical Tree


