CHAPTER 29 Anterior Clinoidal Meningiomas 
INTRODUCTION
Anterior clinoidal meningiomas arise from the meningeal covering of the anterior clinoid process. In the classical neurosurgical literature anterior clinoidal meningiomas have not been separated from medial sphenoid wing or inner sphenoid wing meningiomas. However, accumulating anatomical knowledge and clinical experience has shown that anterior clinoidal meningiomas have unique anatomical and clinical characteristics that puts them apart from meningiomas of the medial sphenoid wing.1–5 Compelling evidence suggests that subtle differences in the patho-anatomy of medial sphenoid wing meningiomas translates into significant differences in surgical outcome. Therefore anterior clinoidal meningiomas should be considered a separate clinical entity. A second level of confusion on the nomenclature stems from the fact that the anterior clinoidal process is situated at the junction of the anterior and middle cranial fossae. Secondary involvement of the anterior clinodial process by anterior or middle fossa meningiomas can create a false impression of primary clinoidal origin. The exact origin of each meningioma can and should be clearly identified. With the help of modern neuroradiology it became increasingly possible to differentiate anterior clinoidal meningiomas. Reported incidence of clinoidal meningiomas ranges from 34%6 to 43.9%7 among sphenoid wing meningiomas.
HISTORY
In 1938, Cushing and Eisenhardt8 broadly classified this group as “deep inner or clinoidal third sphenoid ridge meningiomas,” and this marked the first use of “clinoidal” to distinguish these tumors. In the French literature, Vincent9 referred to them as “sphenocavernous meningiomas” in 1935. The classification of Bonnal and colleagues10 in 1980 identified a group of “sphenocavernous and clinoidal meningiomas” and described them as “extended upward in to the cranial cavity from the dura of cavernous sinus, of the anterior clinoid process and of the internal part of the sphenoid wing.” This group is also similar to the first category of Ojemann’s11 sphenoid ridge meningiomas. Al-Mefty’s1 elegant and more detailed system that was introduced in 1990 classified clinoidal meningiomas as a separate disease entity. Likewise, other reports have attributed unique clinical characteristics and outcomes to sphenocavernous meningiomas (which arise from the lateral wall of the cavernous sinus), cavernous meningiomas (which arise from cavernous sinus proper), planum sphenoidale meningiomas, optic canal meningiomas, and hyperostosing meningiomas of the sphenoid wing.12–16
PRESENTATION
Although the visual problems are the major cause of presenting symptoms in anterior clinoidal meningiomas (45.3%, 53.3%, 58% in some series),2,3,17 this rate is not as high as in other meningiomas located in the neighboring region such as tuberculum sellae meningiomas (75.9%–100%).18–21 The growth potential of the latter tumors may result in early impingement on the optic apparatus. However, for the anterior clinoidal meningiomas, this is true only for Al-Mefty group III tumors that encroach on the optic nerve at the optic foramen.
PREOPERATIVE EVALUATION
Clues to Differentiate Anterior Clinoidal Meningiomas from Other Medial Sphenoidal Ring Meningiomas
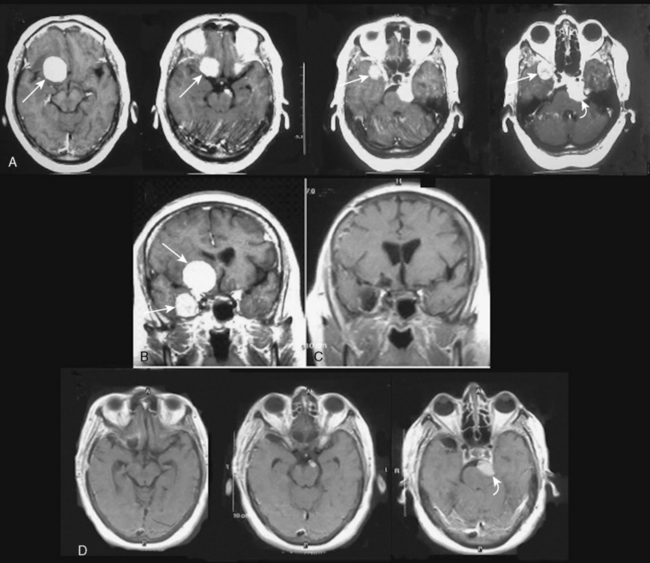
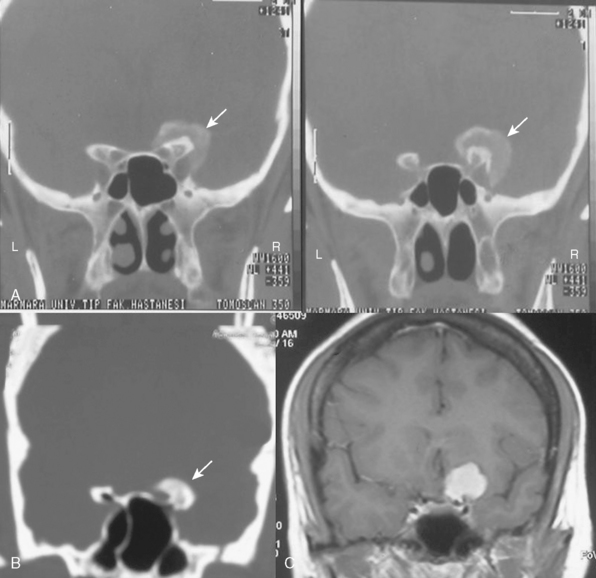
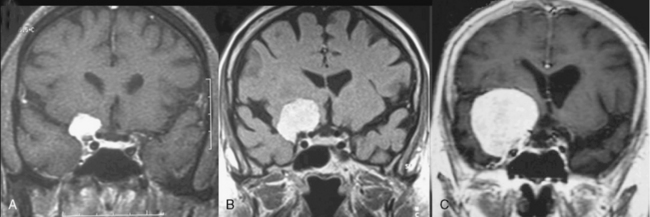
It is difficult to differentiate among meningiomas of this anatomic region before surgery, especially if the tumor is large. However, clues on preoperative imaging can help with diagnosis. With anterior clinoidal meningiomas, the epicenter of the tumor base is on the anterior clinoid process and the tumor typically grows upward, forming a small pedicle toward the suprasellar area and the sylvian fissure. In contrast, meningiomas of the medial third of the sphenoid wing grow in the direction of the anterior aspect of the medial temporal lobe (Fig. 29-1). Another characteristic feature of anterior clinoidal meningiomas is the presence of hyperostosis of the anterior clinoidal process on coronal CT. Accordingly, we recommend coronal CT for any patient with a suspected meningioma at this location (Fig. 29-2).
Cavernous Sinus Invasion
Because anterior clinoidal meningiomas tend to grow upward, true invasion of the cavernous sinus is very rare. The current literature on anterior clinoidal meningiomas documents a very wide range of cavernous sinus invasion rates, ranging from 0% to 44.1%.1–3,22 We believe that this variability is, in part, a reflection of the lack of objective and universal nomenclature among authors. This problem has led to some medial sphenoid wing meningiomas being analyzed as part of the clinoidal group.
Tumor Grading
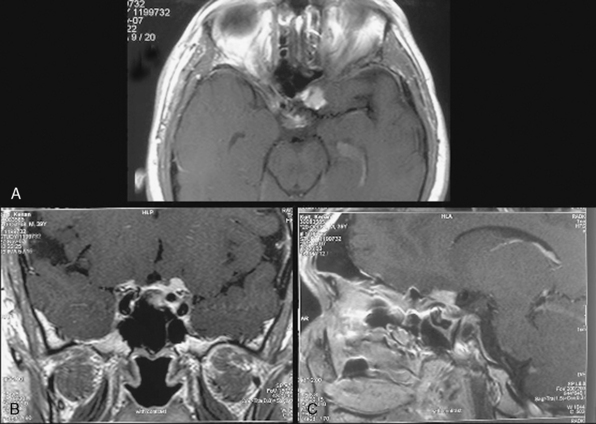
Several classification schemes have been proposed as methods for predicting surgical outcome.1,3,10,20,22 Al-Mefty’s1 elegant classification of clinoidal meningiomas is based on advances in microsurgical anatomy and has been widely accepted. This scheme considers the origin of the tumor and its invasion pattern in the region of the clinoid process as indicators of resectability. It differentiates among lower clinoidal meningiomas (no arachnoidal dissection plane between the internal carotid artery [ICA] and tumor; group I), distal or lateral clinoidal meningiomas (which do have an arachnoidal plane between ICA and tumor; group II), and meningiomas that originate at the optic foramen (group III). In group III tumors, the arachnoidal membrane is present between the ICA and the tumor but may be absent between the optic nerve and the tumor (Fig. 29-3).
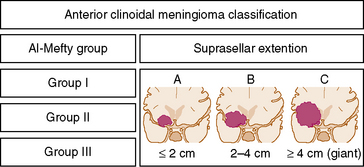
As noted, the current classification scheme considers only tumor origin and invasion pattern around the clinoid process as indicators of resectability.1 However, some reports denote the role of the size in decreasing the success of resection.2,22 Goel and colleagues22 proposed a different method for grading anterior clinoidal meningiomas, one that included tumor size. We wish to emphasize in a very simple and easily remembered manner that pure anterior clinoidal meningiomas grow upward and the size is important. Therefore, we advocate a new classification system that is shown in a simple figure that we think that will be very contributory to the neurosurgical literature. It will also help to reduce the confusion over nomenclature in the current literature. We propose a modification of the classical Al-Mefty system: the addition of subgroups that denote tumor size in coronal plane. This subgrouping can be applied to each of the three groups in the current classification scheme. It should be noted that such absolute cutoff points are irrelevant in biologic systems. This change to the current classification scheme would only provide a more accurate prediction of surgical failure.
According to the new classification the coronal diameter of the tumor is combined with the classical Al-Mefty group designation. Each tumor was graded (typed) with a numerical number denoting the Al-Mefty grouping and a capital letter representing the tumor size on coronal section (Fig. 29-4). A tumor was defined as type A if it measured less than 2 cm, type B if it was 2 cm to 4 cm, and type C (giant) if it was greater than 4 cm (Fig. 29-5). These designations were applied to each group in the current Al-Mefty classification.
Choosing the Optimal Approach
Recent advances in skull-base techniques assisted in resecting these tumors.1–3,22 After operating several cases with pterional and subfrontal approaches, Al-Mefty exclusively used the orbitocranial approach and stated its advantages as: shortest distance to tumor, suitability for surgical attack via multiple routes, and early interception of the tumor’s blood supply through the sphenoid ridge. Many surgeons used various skull-base approaches with or without intra- or extradural removal of anterior clinoid for resecting these challenging tumors. A recent article by Lee and colleagues23 describes a cranial base technique that is a modification of the original “Dolenc approach” and involves extradural clinoidectomy, removal of the roof of the optic canal, and opening of the optic nerve sheath. They stated the advantages of this technique for operating on anterior clinoidal meningiomas and proposed that the conventional pterional approach should be used only for small tumors that cause no visual deficits preoperatively. Mathiesen and Kihlstrom24 also stated that, to achieve or ensure better visual function, it is best to use an extradural approach with drilling of the anterior clinoid and removal of the roof of the optic canal before any intradural steps are performed.
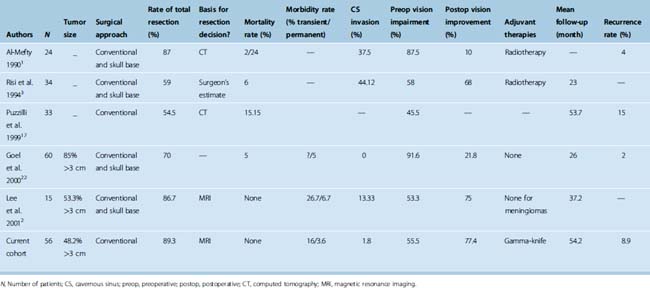
Pure clinoidal meningiomas do not invade the skull base, so the anterior clinoid can be surgically approached with conventional surgical techniques that are fast and efficient and have a relatively low risk of complications. Several reports have documented relatively acceptable results with conventional approaches and, thus, confirm the practical applicability of these techniques.10,20,22,25 Further, two groups of authors who have routinely used skull-base approaches for clinoidal meningiomas stated that conventional techniques would have been sufficient in their cases.3,22 The key features of major series of clinoidal meningiomas published since the introduction of microsurgery are summarized in Table 29-1.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


