♦ Preoperative
Special Equipment
- Patient positioning on a radiolucent table with “bean-bag” facilitates intraoperative x-ray utilization.
Anesthetic Issues
- Anesthesia with muscle relaxation allows greater abdominal wall mobility and minimal muscle contraction during cauterization.
Miscellaneous
- This approach affords satisfactory exposure to the lumbar spine (L2–L5) with minimal risk to the great vessels and viscera. Approaches to right-sided pathology may be more difficult secondary to the size and location of the liver.
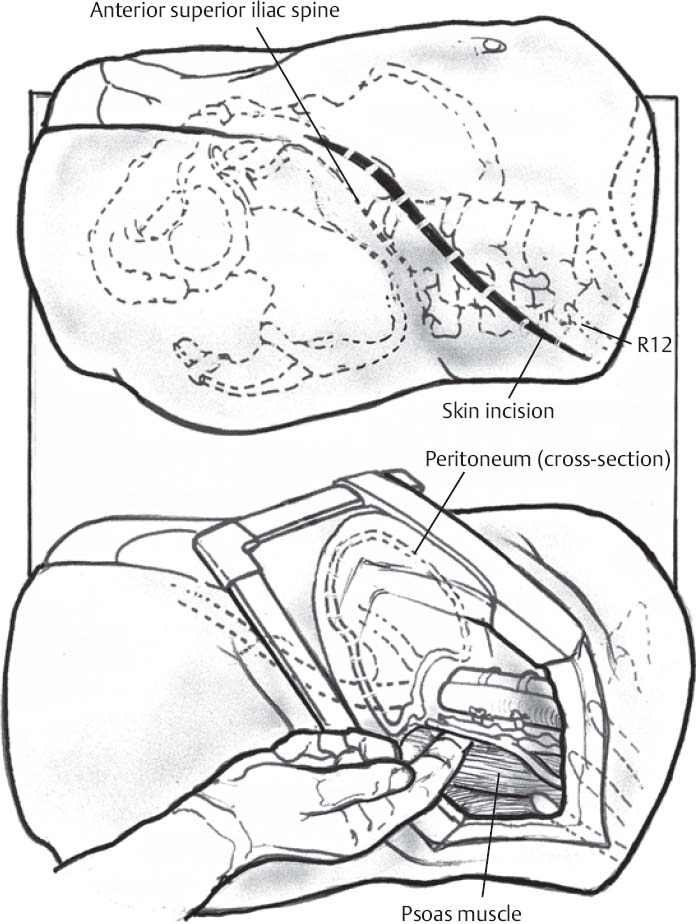
♦ Intraoperative (Fig. 115.1)
Positioning
- The patient is placed in the right lateral decubitus position with an axillary pad and adequate head support. The abdominal and retroperitoneal contents fall dependently toward the contralateral side and facilitate retraction. The knees and hips are flexed slightly to relax the psoas yet minimize anterior interference in the exposure.
- The approach surgeon stands anterior to patient and the assistant stands posterior to the patient. The spine is typically approached from the left, unless the pathology requires a right-sided approach.
Planning of Incision
- Note: “muscle-sparing” and “paramedian” retroperitoneal approaches, as well as exposure to L1–L2 and L5–S1, all require modifications and special considerations that are beyond the scope of this chapter.
- The level of the incision in the craniocaudad plane depends on the level of the spine being approached. Placement of a radiopaque marker (such as a spinal needle) allows placement of the incision directly lateral to the level of pathology.
- The incision should extend medially and transversely in a lazy-S configuration to the lateral edge of the rectus sheath.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


