♦ Preoperative
Operative Planning
- Review of preoperative imaging (magnetic resonance imaging, computed tomography scan)
- Review of angle to L5–S1 disc space as it relates to operative trajectory and the pubic symphysis
Equipment
- General surgery tray
- Vascular instruments: vessel clamps, vessel loops
- Radiolucent table: Jackson table
- Anterior retractor system (e.g., Martin Arms, Thompson–Farley, Synframe [Synthes])
- Fluoroscopy
- Anterior lumbar instruments
Operating Room Set-up
- Headlight
- Loupes
- Fluoroscopy
- Bipolar cautery and Bovie cautery
Anesthetic Issues
- Muscle relaxation during dissection
- Foley catheter
- Preoperative antibiotics
- Decreased positive end expiratory pressure to limit intra-abdominal pressure (if needed)
♦ Intraoperative
Positioning
- Flat on a radiolucent table; a bump may be placed below the buttocks to optimize the trajectory to the L5 and S1 bodies
- It should be possible to obtain anteroposterior and lateral fluoroscopy
- Arms up toward head, angled 90 degrees, or crossed across chest
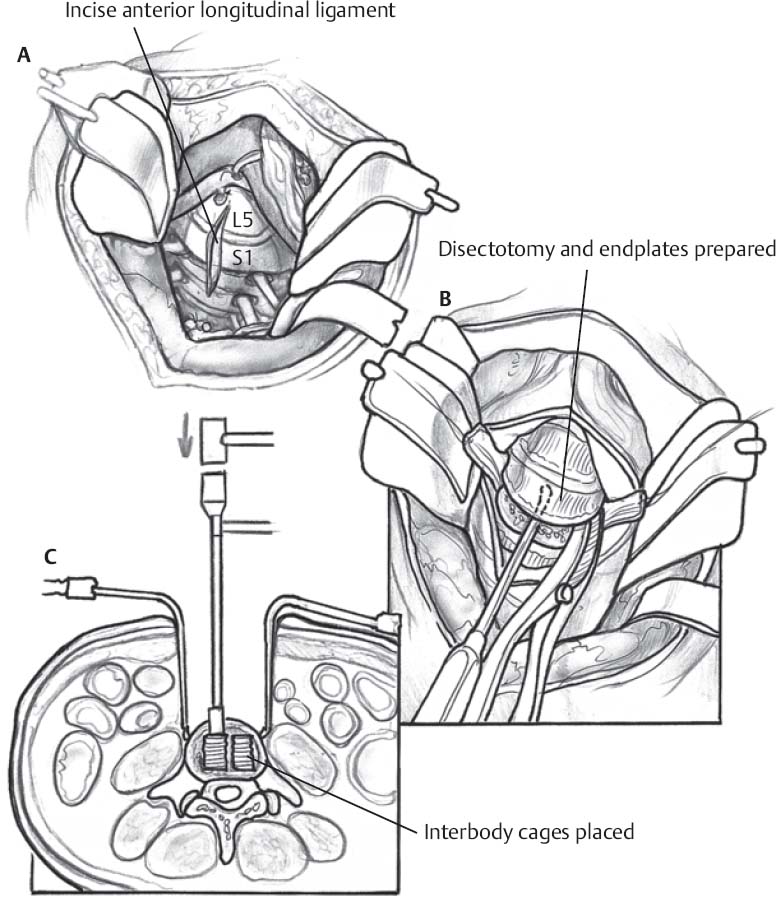
Planning of Incision (Fig. 116.1A)
- Choices include Pfannenstiel, horizontal to midline, or vertical
- Choice of incision is cosmetic and depends on the disc space location
- For L5–S1: incision should be 1 to 2 fingerbreadths above the pubic symphysis
- For L4–L5: a vertical incision may be more appropriate
Dissection (Fig. 116.1B)
- Bovie cautery down to anterior rectus sheath
- Open the sheath in line with the incision to expose the two halves of the rectus muscle.
- Retract the rectus muscle laterally to expose the transversalis muscle and fascia.
- Make a small hole in the peritoneum; make sure no bowel is present within the forceps.
- Open the peritoneum widely.
- Retract small bowel and mesentery superiorly (pack with moist sponges)
- Retract the sigmoid colon caudally and to the left to expose the posterior peritoneum.
- Elevate the posterior peritoneum with forceps and make a sharp incision.
- Visualize and palpate the aorta and vena cava prior to opening the posterior peritoneum, as well as the sacral promontory.
- After splitting the peritoneum, perform blunt dissection with a Kittner swab to identify the disc space and vertebral bodies.
- Identify, mobilize, and ligate the middle sacral artery.
- Mobilize the left common iliac vein and right common iliac artery off the L5–S1 disc space with the Kittner, if necessary.
- The vessels may then be held in retraction with a retractor set or handheld retractors.
- For L4–L5, one may be able to work through the vascular “V” as described, or the vessels may have to be retracted laterally.
- Care must be taken to identify the iliolumbar vein and ligate it prior to extensive mobilization of the vessels.
Disk Removal (Fig. 116.1C)
- Confirm the disc space with fluoroscopy.
- Incise the disc with a no. 10 scalpel blade on a long handle.
- Large curettes and rongeurs may be used to complete the discectomy.
- Continue the discectomy to the posterior annulus and vertebral body—this may be confirmed with fluoroscopy.
- Perform appropriate bone grafting or cage placement at this point.
Only gold members can continue reading. Log In or Register to continue







