Anxiety
INTRODUCTION
Anxiety is part of a mechanism developed in higher animals to handle adverse situations. The anxiety response can be conceptualized as part of the brain’s alarm system firing during times of perceived danger. The characteristic responses including avoidance, hypervigilance, and increased arousal are implemented to avoid harm.
The evolutionary drive to survive has invariably enhanced a strong anxiety response. Unfortunately, in many individuals, that mechanism is overactive. The alarm fires too frequently. Such people cannot seem to turn down their internal alarm even when the coast is clear.
Diagnostic and Statistical Manual
The Diagnostic and Statistical Manual (DSM) system categorizes anxiety into a multitude of different disorders (generalized anxiety disorder [GAD], obsessive-compulsive disorder [OCD], post-traumatic stress disorder [PTSD], etc.). Although each disorder has unique clinical features, it is not clear whether they actually describe different pathologic states. The disorders have the following similar characteristics:
Most patients with an anxiety disorder will have features of the other disorders.
Many of the disorders respond to similar treatment interventions: selective serotonin reuptake inhibitors, benzodiazepines, exposure therapy, and so on.
There is little evidence to show that different disorders stem from different regions of the brain.
We believe the reaction to perceived threat is mediated in similar pathways in the brain in patients with various anxiety disorders. The one potential exception is OCD, which has unique mechanisms in the brain and will be reviewed separately.
Acute Stress
The body’s reaction to an acutely stressful situation is well known to all of us. The characteristic rapid heart rate, dry mouth, and sweaty palms are the body’s response to increased sympathetic activity generated by a stressful situation (see Figure 2.8). Less readily apparent are the endocrine responses to acute stress.
In the late 1970s, Ursin et al. studied the endocrinologic responses of young Norwegian military recruits during parachute training. During the exercise, the recruits repeatedly jumped off a 12 m tower and slid down a long sloping wire to learn the basic skills of parachuting. The training was designed to give the jumper a realistic sensation of the initial free fall. Measures of anxiety and performance skill as well as serum hormone levels were captured at baseline and after each jump.
Initially, anxiety was high and performance was poor. As the days and number of jumps progressed, anxiety subsided and the skills improved. The endocrinologic measures are shown in Figure 22.1. Presumably, the anxiety induces changes in the releasing hormones, which alter the pituitary hormones and ultimately the peripheral hormones (see Figure 7.4). Note how testosterone levels drop with the stress of the jumping, while the other measures increase. Likewise, all return to baseline as the recruits habituate to the task.
While the average individual shows a peak in the endocrine response at the start of a difficult task, which usually subsides as the person gains mastery, this is not true for everyone. Some people have more exaggerated and persistent endocrine reactions. Kirschbaum et al. looked at salivary cortisol levels in 20 men exposed to 5 consecutive days of public speaking. For the total group, the average cortisol levels jumped on the first day and then gradually declined over the following days. However, the men
could be divided into two groups: high responders and low responders. Figure 22.2 shows the cortisol levels for these two groups.
could be divided into two groups: high responders and low responders. Figure 22.2 shows the cortisol levels for these two groups.
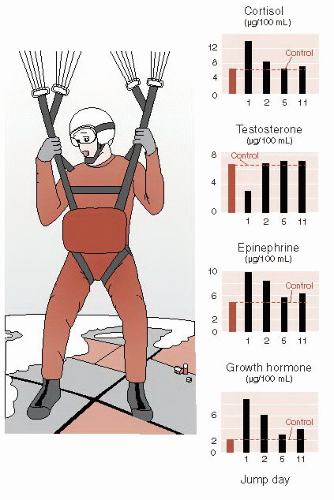 FIGURE 22.1 • The stress of learning to parachute, on young recruits, results in changes in hormones, which return to baseline as the anxiety decreases. (Adapted from Rosenzweig MR, Breedlove SM, Watson NV. Biological Psychology. 4th ed. Sunderland, MA: Sinauer; 2005. Graphs adapted from Ursin H, Baade E, Levine S. Psychobiology of Stress: A Study of Coping Men. New York, NY: Academic Press; 1978.) |
Note how the cortisol in the low responders peaked the first day, but then quickly returned to baseline levels on the following days. These individuals appear to adjust rapidly to the stress of public speaking. The high responders, on the other hand, showed higher, more persistent peaks of cortisol. Such people appear to have a harder time turning off the stress response. Presumably, they have a stronger alarm response originating in the brain, which is driving this endocrine reaction. Alternatively, they have a weak or faulty regulatory system that governs or turns down the response. Or there could be elements of both in some people.
Cortisol has been implicated as a culprit in the development of anxiety after trauma, although not everyone agrees if it is too much or too little. Some researchers believe excess cortisol sensitizes the amygdala and are using mifepristone (RU-486, the “abortion pill”) to block the glucocorticoid receptors after a traumatic event. Other researchers believe the traumatic consolidation of memories is enhanced by insufficient cortisol and they are giving cortisol to patients acutely after trauma to prevent the development of PTSD. Both groups have produced small pilot studies with positive results. The impending larger trials should clear up this paradox.
NEURONAL CIRCUITRY
Multiple lines of research identify the prefrontal cortex (PFC), amygdala, hippocampus, and hypothalamic-pituitary-adrenal (HPA) axis as the regions involved with anxiety (Figure 22.3). However, if there is one organ that represents an alarm system in the brain, it is the amygdala (see Figure 2.7).
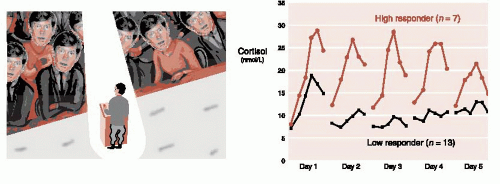 FIGURE 22.2 • Men stressed by public speaking over 5 consecutive days showed different patterns of adrenocortical response. (Graph adapted from Kirschbaum C, Prussner JC, Stone AA, et al. Persistent high cortisol responses to repeated psychological stress in a subpopulation of healthy men. Psychosom Med. 1995;57(5):468-474. Illustration adapted from Images.com.) |
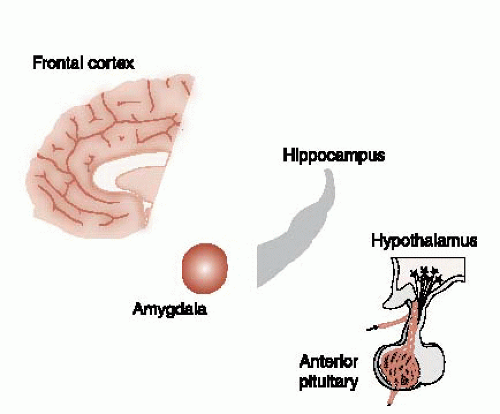 FIGURE 22.3 • The important regions of the brain affecting anxiety. |
Amygdala
In their classic studies with rhesus monkeys in the 1930s, Heinrich Klüver and Paul Bucy identified the amygdala as a structure that is essential for the expression of numerous emotions. They removed large segments of the temporal lobes from wild monkeys and transformed the monkey’s temperament. Aggressive and easily frightened monkeys were changed into docile, calm creatures.
The monkeys virtually became tame. They did not react fearfully to strange humans or even a snake. Of particular interest, the monkeys failed to learn from negative experience. One monkey, bitten by a snake, later approached a snake again as if nothing had happened—a clear example of the survival value of anxiety. The entire constellation of symptoms is called the Klüver-Bucy syndrome and includes a host of other bizarre features, such as hypersexuality and a tendency to transfer objects to the mouth.
In the intervening years, it has been demonstrated that the emotional changes of the Klüver-Bucy syndrome can be elicited with the removal of just the amygdala. Other evidence points to the amygdala as an important region in the recognition and management of fear:
Electric stimulation of the amygdala in animals elicits fearful behavior, for example, freezing and tachycardia.
Humans with damaged amygdala exhibit impaired fear conditioning.
Functional imaging studies of humans show activation of the amygdala during fear learning.
Recognizing Danger
Sensory information enters the brain by way of the thalamus. All neurons carrying auditory and visual information synapse first in the thalamus before being relayed to the appropriate cortical region for analysis. Information about danger is particularly important and needs to be recognized quickly. Work by LeDoux et al. at New York University has shown that the amygdala quickly receives some preliminary information about dangerous events even before it is processed in the cortex.
Figure 22.4 shows an example of a person coming upon a rattlesnake. This life-threatening visual information proceeds from the eyes to the thalamus. However, the thalamus sends fast but rudimentary signals to the amygdala at the same time that the full information is passed back to the visual cortex. The amygdala in turn sends responding signals to the muscles, sympathetic nervous system, and hypothalamus. The person jumps even before being consciously aware of what has been seen. LeDoux has shown with rats that the fear response is preserved even if the neural connections between the thalamus and the cortex are cut. In essence, the animal startles without knowing why.
We all have had the experience of being frightened when seeing something, only to realize that it was just a rope or shadow—not a real threat. It is the fast track from the thalamus directly to the amygdala that causes the false alarm. This is considered to be “unconscious” or preconscious. We jump before we are aware. Patients with anxiety disorders can have exaggerated startle responses. They are burdened with an exaggerated, unconscious reaction to what are actually harmless events.
Anticipatory Anxiety
Some people dread personal interactions in which they will be the focus of attention. Typically, they fear they will embarrass themselves. The anticipatory anxiety can ultimately restrict what they do and limit their social life and career path.
An imaging study looked at the activity in the brain of such patients who were asked to anticipate making a public speech. By subtracting the activity during anticipation from that at rest, they identified the areas of activity. Patients showed greater activity in their amygdala as well as hippocampus and insula. Figure 22.5A shows the functional magnetic resonance imaging (fMRI) slice at the level of the amygdala.
Anticipatory anxiety is not all bad. Figure 22.5B shows the hypothetical upside down U curve that many think represents the benefits and problems with anticipatory anxiety. Some anxiety is beneficial and
actually improves performance; however, too much of it is overwhelming and results in a poorer outcome.
actually improves performance; however, too much of it is overwhelming and results in a poorer outcome.
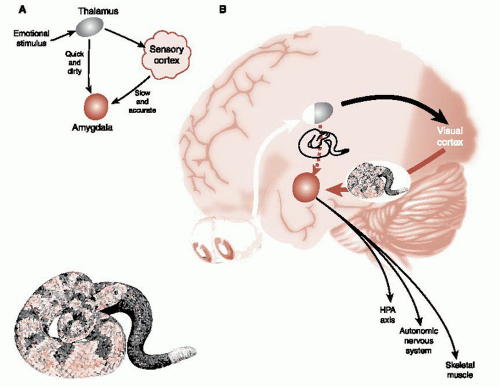 FIGURE 22.4 • Two representations showing the two tracks that emotionally stimulating sensory information takes to the amygdala after entering the brain through the thalamus. HPA, hypothalamic-pituitary-adrenal. (Adapted from LeDoux JE. Emotion, memory and the brain. Sci Am. 1994;270(6):50-57.) |
Amygdala Memories
There is evidence that primitive emotionally relevant memories are stored in the amygdala. For example, in rodents:
Long-term potentiation (LTP) can be induced in the amygdala;
Protein synthesis inhibitors injected directly into the amygdala will prevent the formation of fear conditioning; and
Chronic stress will induce increased dendritic branching in the amygdala.
These results suggest that the typical structural changes that are observed with memory formation occur in the amygdala in reaction to fearful circumstances. This may be one reason why traumatic events are so persistent. Fearful experiences form quickly, and enduring memories then reside in both the neocortex and the amygdala.
Prefrontal Cortex
One of the central components of anxiety is the feeling that one is not in control. Patients will complain of increased anxiety when they lose control, for example, when the door closes on an airplane or when their social support drives off—anytime they feel trapped. Feeling in control, on the other hand, calms anxiety. The ability to reappraise a difficult situation into more
favorable terms is a function of executive control. Rational reappraisal is a central feature of CBT.
favorable terms is a function of executive control. Rational reappraisal is a central feature of CBT.
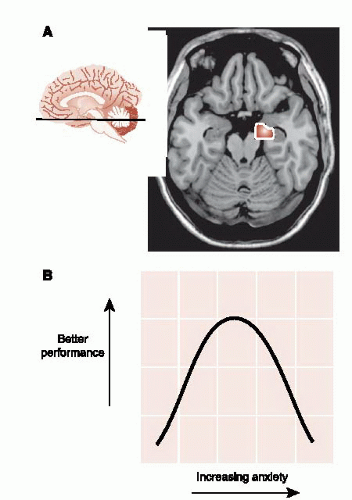 FIGURE 22.5 • A. Increased activity at the level of the amygdala when patients with anxiety anticipate making a public speech. B. Hypothetical upside down U curve showing benefits and problems of anticipatory anxiety. (Functional magnetic resonance imaging from Lorberbaum JP, Kose S, Johnson MR, et al. Neural correlates of speech anticipatory anxiety in generalized social phobia. Neuroreport. 2004;15(18):2701-2705.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|




