Chapter 31 Applied Anatomy of the Cervical Spine
Spinal Column
Occipitocervical Junction
Osseous Elements
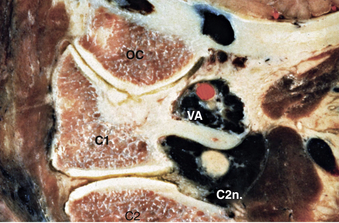
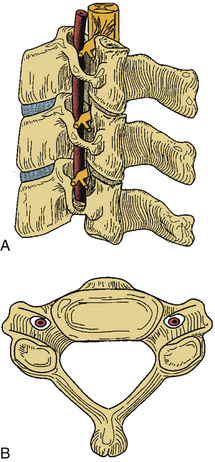
The first and second vertebral segments attach to the occiput to form the craniocervical junction, which is a complex articular system permitting rotational and nutational movement. The first cervical segment, also known as C1 or the atlas, is composed of a ventral and dorsal arch, joined laterally by symmetrical lateral masses (Figs. 31-1 to 31-3). The superior and inferior articulating surfaces of the lateral mass are concave to enable articulation with the occipital condyles, superiorly, and the shoulders of the axis, inferiorly (Figs. 31-4 and 31-5). The ventral arch forms a short bridge between the lateral masses, with a dorsal articular surface forming a synovial joint with the odontoid process of C2 and an anterior tubercle ventrally to which the longus colli muscle attaches. The dorsomedial walls of the C1 lateral masses form a small tubercle that serves as the attachment for the transverse atlantoaxial ligament. The dorsal arch of the atlas typically forms a posterior tubercle in the midline that is a rudimentary equivalent to subaxial spinous processes. Caution should be exercised in dissection of this structure because the dorsal arch may be incomplete. The dorsal arch is round in cross-section in the midline and attenuates laterally to form a flatter surface where it attaches to the dorsal lateral masses. The superior surface of the lateral dorsal arch forms a groove known as the sulcus arteriosus on which the vertebral arteries run bilaterally; it is often thin or even dehiscent and great care must be taken when exposing the inferior surface of the C1 lateral mass. The lateral masses are bounded laterally by short transverse processes that are fenestrated by the transverse foramen, or foramen transversarium. As in the subaxial spine, the vertebral artery traverses the transverse foramen of C1 before turning 90 degrees medially to run along the superior surface of the dorsal arch, as described previously. This genu lies 1.5 to 2 cm lateral to midline1 and dorsal dissection should seldom require exposure of this precarious region.
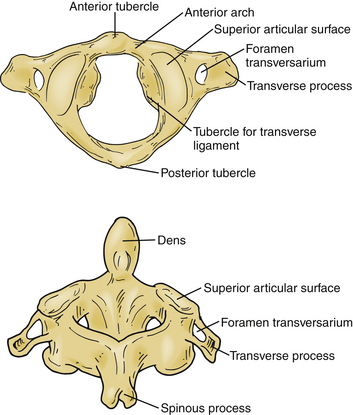
The second vertebral segment, or axis (see Figs. 31-1 to 31-4), is a distinctive osseous structure. The odontoid process, a peglike rostral projection, forms a synovial joint with the atlas along its ventral border and allows the atlas to rotate on C2, with translational restriction created by a complex of ligamentous structures. The tip of the odontoid process serves as the attachment for the apical ligament, which connects C2 to the basion (the ventral lip of the foramen magnum). The tip is flanked by two bony prominences that serve as the attachments for the paired alar ligaments that span the divide between C2 and the occipital condyles. The transverse atlantoaxial ligament traverses the dorsal border of the odontoid process, which often carries a groove for this strong ligament. The neck of the odontoid process narrows to meet the vertebral body of C2 and is a common site for C2 fracture. The vertebral body culminates rostrally to form two bilaterally symmetrical “shoulders” that flank the odontoid process and articulate with the lateral masses of C1. A relatively long pars interarticularis spans the interval between superior and inferior articulating processes and is laterally bounded by the transverse process of C2. The disproportionate length of the C2 pars interarticularis has important clinical implications. Because the superior and inferior articulating processes of C2 are coronally offset, extension applies significant strain on the C2 pars interarticularis. Under forceful hyperextension, the pars interarticularis may fracture, giving rise to the mechanism and morphology of the so-called hangman’s fracture. As at other levels, this process is fenestrated by the transverse foramen, which lies immediately lateral to the C2 pedicle and serves as the conduit for the vertebral artery. Unlike at other levels, the C2 foramen is angulated 45 degrees laterally so that the vertebral artery is partially roofed by the superior articular process.2 The inferior articular process forms an articulation with the C3 superior articular process and assumes the more typical orientation of subaxial lateral masses.
Ligamentous Structures
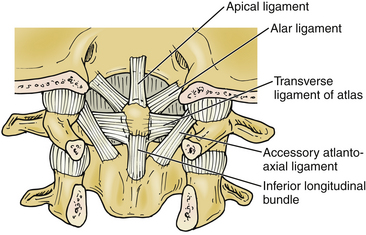
Although the articular surfaces of the occipitocervical junction are oriented to permit constrained flexibility, a complex of intervening ligamentous structures acts in concert to restrict excessive translation and rotation (see Figs. 31-2 to 31-4). Three ligaments span the divide between the odontoid process and the occiput. In the midline, the apical ligament spans the interval between the basion and the tip of the odontoid process. This ligament, also known as the middle odontoid ligament or suspensory ligament, is of unclear biomechanical significance because it has been described as absent in 20% of specimens.3 The alar ligaments are bilaterally symmetrical structures approximately 1 cm in length spanning from the dorsolateral odontoid tip to the medial occipital condyles. Each alar ligament restricts excessive rotation to the contralateral side and excessive lateral bending to the contralateral side.4
The cruciate, or cruciform, ligament is the most important ligamentous structure of the craniovertebral junction. It is composed of four limbs that unite over the dorsal odontoid process. The superior limb, or ascending band, inserts on the occiput, whereas the inferior limb, or descending band, inserts on the dorsal body of C2. The transverse atlantoaxial ligament forms the transverse limbs of this complex and attaches to bony tubercles on the medial borders of the C1 lateral masses. The transverse ligament is a strong, inelastic structure composed of primarily dense collagen with a ventrolateral transition to fibrocartilaginous tissue near its insertion on the C1 lateral masses. As a consequence, this lateral transition portion is the zone most susceptible to traumatic rupture, and the transverse atlantoaxial ligament has been demonstrated to rupture under loads of 400 to 1100 N.5 Rupture of this ligament may be identified on MRI, particularly on gradient-echo sequences,6 and is associated with atlantoaxial instability. On occasion, the insertion of this ligament will fracture off the medial wall of one or both lateral masses while the ligament itself remains intact. CT and MRI characterization of these disruption patterns has important implications for the management of traumatic atlantoaxial instability.
Subaxial Cervical Spine
Osseous Structures
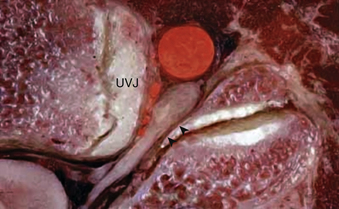
Each vertebral segment can be divided into a ventral portion, the vertebral body, and a dorsal portion, the dorsal or vertebral arch. The cervical vertebral body is roughly cylindrical in geometry, although the anteroposterior diameter is typically smaller than the transverse diameter. Relative to the vertebral arch, the cervical vertebral bodies are smaller than the vertebral bodies of the thoracolumbar spine, likely because they bear significantly less load. The superior and inferior surfaces of the vertebral body serve as the superior and inferior end plates, respectively. The lateral edges of the superior end plate curve sharply upward to form the uncinate processes bilaterally, a unique feature of the cervical spine. These processes articulate with complementary bevels on the lateral surfaces of the adjacent inferior end plate. Although this articulation is referred to as the “uncovertebral joint,” it contains no synovial fluid and as a consequence is not a true joint7 (Figs. 31-6 and 31-7).


The most distinctive feature of the cervical spine is the fenestration of the transverse processes that flank each vertebral body. The transverse process projects ventrolaterally with a deep groove along its superior surface; this serves to carry the cervical spinal nerves. The transverse process terminates laterally with two prominences—the anterior and posterior tubercles. The anterior tubercle serves as an attachment for the ventral cervical musculature and the posterior tubercle serves as an attachment for the dorsal cervical musculature. The transverse foramen, or foramen transversarium, fenestrates the transverse process and carries the vertebral arteries bilaterally (Figs. 31-8 to 31-10).

Importantly, the cervical pedicle serves as the dorsomedial wall of the foramen transversarium, exposing the vertebral artery to hazard when pedicle screws breach laterally. The cervical pedicles connect the dorsal arch with the vertebral body and are angled medially between 38 and 48 degrees from the midsagittal plane.8 The pedicles of C3 through C7 range in outer diameter from 6.0 to 6.5 mm9 and in inner diameter from 2.7 to 3.1 mm.8 The pedicle is thinnest along its lateral wall. In aggregate, these features make safe placement of cervical pedicle screws a challenge. The medial wall is close to the thecal sac, the lateral wall is close to the vertebral artery, and the superior wall is close to the superjacent nerve root.
The superior and inferior articular processes of the cervical spine are oriented obliquely on sagittal projection, with complementary surfaces on adjacent segments. Together with the intervening bone, these articular processes combine to form lateral masses at each level that are parallelogram-shaped in sagittal cross-section. Adjacent lateral masses in the subaxial cervical spine are in close apposition so that in aggregate they form a flexible, cylindrical column of bone dorsolateral to the vertebral bodies. This pillar-like architecture affords axial load-bearing capacity to the dorsal vertebral arches. The oblique configuration of articular surfaces imparts a shingle effect to the lateral masses and allows for flexion and extension while restricting translation, affording osseous neuroprotection for the enveloped cervical spinal cord and nerve roots (see Fig. 31-6). The lateral mass serves as a common anchor point for instrumentation, but an awareness of adjacent neurovascular structures is essential for safe placement of lateral mass screws that avoid the vertebral artery and cervical nerve roots. A rostral screw trajectory is protective of the exiting nerve root, whereas a lateral trajectory protects the vertebral artery (Figs. 31-11 to 31-13).

Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


