Chapter 76 Assessing needs
The health services are constantly in a state of flux due to alterations at the supply side of care, for example, the appearance of new drugs, the introduction of new medical technology and attempts to make services more efficient and effective. Health services are also changing through alterations in demand, for example, the changing composition of the population, as people live longer (see pp. 16–17), migration flows change (see pp. 48–49) or new diseases appear (HIV/AIDS in the late 20th century) and preferences and expectations among consumers change for certain kinds of treatment. Somewhere in this pool of potentially conflicting interests we have to establish the needs of individuals, communities and populations whilst ensuring that each receives maximum benefit within the limits of available resources, such as staff, buildings and funding (Powell, 2006).
The need for needs assessment
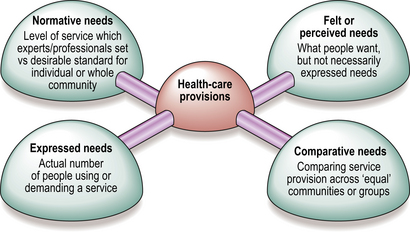
Why does a service provider, a policy-maker, a doctor or a hospital manager set about identifying the needs of people? Providers of health care need to know: (1) what users need in the way of health care; and (2) what is needed in a particular area, in order to achieve an improvement in the health of the population. These two objectives are not the same. What potential or actual service users feel they need (Fig. 1) might only partially overlap with what policy-makers consider to be the best possible range of services in an area that can improve the health of the people there (normative needs). Both types have to be distinguished from expressed needs, the actual use or demand for a service, and comparative needs, which compare services across similar communities or client groups; for example, comparing the services available to people with HIV and those with cancer, or comparing services available in New York with those in Washington DC. Thus need is not a unified concept.