Because the neurologic system is so complex and intricate, evaluating it may seem daunting. However, routine tests for assessing neurologic status, although extensive, are basic and straightforward. In fact, you may include some of these tests in your daily practice.
Just talking with a patient helps assess his orientation, level of consciousness, and ability to formulate and produce speech. Having him perform a simple task such as walking allows you to evaluate motor ability. Further, knowledge of neurologic anatomy, physiology, and assessment will enhance patient care and may save a patient from irreversible neurologic damage. If possible, you should start with taking a thorough health history and then proceed with performing a complete physical assessment.
HEALTH HISTORY
Begin the health history by asking about the patient’s chief complaint. Then gather details about his current illness, past illnesses, family history, drug history, and psychosocial history. Also perform a body systems review.
If possible, include the patient’s family members or close friends when taking the history. Don’t assume that the patient remembers accurately; corroborate the details with others to get a clearer picture.
AGE AWARE
When obtaining a child’s health history, ask questions about the child’s development, including a prenatal history up to the present. Also evaluate the child’s achievement of developmental milestones, such as sitting up, walking, and talking at the appropriate age.
Chief complaint
The most common complaints about the neurologic system include headache, dizziness, disturbances in balance and gait, and changes in mental status or level of consciousness (LOC).
When documenting the patient’s chief complaint, record the information in the patient’s own words. Ask him about the problem’s onset and frequency, what precipitates or exacerbates it, and what alleviates it. Also ask whether other symptoms accompany the problem.
Current health history
Ask the patient to elaborate on his chief complaint, using questions to focus the interview. Determine if he’s experiencing problems with his activities of daily living (ADLs) due to the complaint. Also question the patient about measures used to treat the problem and if he experienced any adverse effects from those treatments.
Make sure you ask about other aspects of his current health. Help the patient describe problems by asking pertinent focused questions.
AGE AWARE
Keep in mind that some neurologic changes, such as decreased reflexes, hearing, and vision, are a normal part of aging. Additionally, because neurons undergo various degenerative changes, aging can lead to diminished reflexes; decreased hearing, vision, taste, and smell; slowed reaction time; decreased agility; decreased vibratory sense in the ankles; and the development of muscle tremors, such as in the head and hands. Remember that not all neurologic changes in elderly patients are caused by aging and that certain drugs can cause changes as well. Find out if the changes are symmetric, indicating a condition, or if other abnormalities need further investigation.
HEADACHE
Ask the patient whether he has headaches. If so, ask him how often they occur and what seems to provoke them. Find out if light bothers his eyes during a headache. Also find out what other symptoms occur with the headache.
AGE AWARE
In children older than age 3, headache is the most common symptom of a brain tumor. In a school-age child, ask the parents about recent scholastic performance and about any problems at home that may produce a tension headache. Twice as many young boys have migraine headaches than girls.
Attempt to gather additional information about the headache to aid in ascertaining the possible cause. First, ask the patient where the pain is located, such as across his forehead, on one side of his head, or at the back of his head and neck. Pain that emanates from specific areas of the head characterizes certain types of headaches. For example, tension headaches are usually located in the occipital area, and migraine pain tends to be unilateral.
Ask the patient if the pain is tight, bandlike, boring, throbbing, steady, or dull. Headaches can be identified by the quality of pain they produce. A dull, steady pain may indicate a tension, or muscle, headache; severe or throbbing pain may indicate a vascular problem such as a migraine headache.
Find out from the patient if the pain’s onset is sudden or gradual. Migraine headaches may develop suddenly, with no warning, but are usually preceded by a prodromal disturbance. Headaches associated with hemorrhage typically occur suddenly and with increasing severity.
Ask the patient how long the pain usually lasts and if it’s continuous or recurrent. Tension and migraine headaches may last from several hours to several days. Cluster headaches last about an hour. Also, find out if the headaches are occurring more frequently because a change in headache pattern may signal a developing condition.
Next, find out when the headaches occur, such as in the evening or if they wake him during the night. Although tension headaches usually occur in the evening, a patient may awaken in the morning with such a headache. A patient who suffers from headaches caused by hypertension, inflammation, or tumors may awaken anytime with the pain. Cluster headaches typically awaken the patient a few hours after he has fallen asleep.
Ask the patient if he sees flashing lights or shining spots or feels tingling, weakness, or numbness immediately before the headache occurs. These are common characteristics of the prodromal (premonitory) neurologic disturbance that commonly precedes a migraine headache.
Ask the patient if the pain worsens when he coughs, sneezes, or bends over. Valsalva’s maneuver may exacerbate a headache caused by an intracranial lesion such as a subarachnoid hemorrhage. Find out if he becomes nauseated or vomits during the headache. Such GI distress may accompany a migraine headache, a brain tumor, or hemorrhage.
Headaches that occur daily for a prolonged period may be related to stress or depression. Ask the patient if he’s been experiencing these difficult feelings.
Find out about any measures, such as medication, he takes for the headache and whether it’s effective. Ask about other therapeutic approaches, such as lying down, applying heat, or sleeping, and if they relieve the headache.
Finally, have your patient describe the last headache he experienced by rating it on a scale of 1 to 10 with 1 being no pain and 10 being the worst headache he has ever had. How a particular headache differs from headaches a patient typically experiences can provide valuable clues to the possible cause.
DIZZINESS
Ask the patient about complaints of feeling dizzy. Find out if he has dizziness, numbness, tingling, seizures, tremors, weakness, or paralysis. Ask how often it occurs and how long each episode lasts. Find out if the dizziness abates spontaneously or if it leads to loss of consciousness. Ask him if the dizziness is triggered by sitting or standing up suddenly or stooping over. Find out if being in a crowd makes the patient feel dizzy. Ask about emotional stress. Find out if the patient has been irritable or anxious lately. Ask him if he has insomnia or difficulty concentrating. Look for fidgeting and eyelid twitching. Observe the patient to see if he startles easily. Also, ask about palpitations, chest pain, diaphoresis, shortness of breath, and chronic cough.
BALANCE AND GAIT DISTURBANCES
Find out if the patient has problems with walking and keeping his balance. Then ask him when his balance or gait impairment first developed and whether it has worsened recently. Find out if the problem occurred gradually over time or developed suddenly. If he has difficulty remembering, attempt to gain information from family members or friends. Find out if the problem has remained constant or if it’s getting progressively worse. Ask about environmental changes such as hot weather, or other conditions, such as fatigue or warm baths or showers that could make his problem worse. Such exacerbation typically is associated with multiple sclerosis. Also, find out if anyone in his family has experienced a similar type of problem.
MENTAL STATUS OR LOC CHANGES
Ask the patient how he would rate his memory and ability to concentrate. Ask him if he ever has trouble speaking or understanding people. Find out if he has difficulty reading or writing. If so, find out how much the problems interfere with his ADLs.
If the patient complains of problems with mental status, such as confusion, ask him how long he has felt confused and how quickly it occurred. Depending on the patient’s degree of change, family members may need to be questioned to determine the true nature of the problem. Find out if the change occurred gradually or developed suddenly. An acute onset of confusion can indicate metabolic encephalopathy or delirium; gradual onset usually indicates a degenerative disorder. Ask if the confusion fluctuates. This question can help distinguish between an extracerebral disorder, such as metabolic encephalopathy, and a subdural hematoma caused by intracerebral impairment, such as arteriosclerosis or senile dementia.
If the patient was found unconscious, note where he was found. This answer may provide clues to the cause of the unconsciousness such as a possible reaction to drugs or alcohol. Ask him if unconsciousness occurred abruptly or gradually. Find out if his LOC has fluctuated. Abrupt change in LOC may indicate a stroke. Gradual onset could result from metabolic, extracerebral, toxic, or systemic causes.
A fluctuating LOC may indicate that systemic hypotension is affecting the brain. Find out from the patient what may have served as a trigger to exacerbate an existing condition, resulting in unconsciousness. For example, an infection or a break in treatment of an existing condition can result in unconsciousness.
Drug history
Obtain a thorough drug history, including medication type and dosage. Ask the patient if he has been taking over-the-counter medications, herbal supplements, vitamin supplements, or illegal substances. Find out if the patient has been taking the medication as prescribed. Ask him if any medications are newly prescribed and how they make him feel. Also find out about alcohol intake, frequency, and amount, and type of alcohol ingested.
Past health history
Explore all of the patient’s previous major illnesses, recurrent minor illnesses, accidents or injuries, surgical procedures, mental illness, and allergies. Establish when his last physical examination occurred and if any routine examinations, such as an eye examination, took place. Ask about dietary habits and restrictions. Find out if he exercises daily. Ask him if he currently smokes or uses tobacco products or has smoked in the past. Calculate a pack-per-year history. Find out if the patient has ever attempted to stop smoking or using tobacco.
Family history
Information about the patient’s family may help uncover hereditary disorders. Ask him if anyone in his family has had diabetes, cardiac or renal disease, high blood pressure, cancer, bleeding disorders, mental disorders, or a stroke.
Some genetic diseases are degenerative; others cause muscle weakness. For example, seizures are more common in patients whose family history shows idiopathic epilepsy, and more than 50% of patients with migraine headaches have a family history of the disorder.
Psychosocial history
Always consider the patient’s cultural and social background when planning his care. Note his ethnic background and if it’s a factor in his daily living. Find out what religion he practices and if he actively practices his beliefs. Also note the patient’s education level and occupation. Find out if he has a stable or erratic employment history. Find out if his employment involves possible exposure to toxic substances, such as heavy metals or carbon monoxide. Ask him if he lives alone or with someone and what type of dwelling he lives in, and find out if he has a support system. Find out what his hobbies are. Ask him how he views his illness. Ask if the patient needs assistance with financial matters. Assess the patient’s self-image while gathering this information.
PHYSICAL ASSESSMENT
A complete neurologic examination can be time-consuming and detailed, making it difficult to perform one in its entirety. However, if the initial screening examination suggests a neurologic problem, you may want to perform a more detailed neurologic assessment.
Always examine the patient’s neurologic system in an orderly fashion.
Vital signs
The central nervous system (CNS), primarily by way of the brain stem and the autonomic nervous system (ANS), controls the body’s vital functions, including body temperature; heart rate and rhythm; blood pressure; and respiratory rate, depth, and pattern. However, because these vital control centers lie deep within the cerebral hemispheres and in the brain stem, changes in these vital signs aren’t usually early indicators of CNS deterioration. When evaluating the significance of vital sign changes, consider each sign individually as well as in relation to the others.
TEMPERATURE
Normal body temperature ranges from 96.7° F to 100.5° F (35.9° C to 38.1° C), depending upon the route used for measurement. Damage to the hypothalamus or upper brain stem can impair the body’s ability to maintain a constant temperature, resulting in profound hypothermia (temperature below 94° F [34.4° C]) or hyperthermia (temperature above 106° F [41.1° C]). Such damage can result from petechial hemorrhages in the hypothalamus or brain stem; trauma, causing pressure, twisting, or traction; or destructive lesions.
HEART RATE
Because the ANS controls heart rate and rhythm, pressure on the brain stem and cranial nerves slows the heart rate by stimulating the vagus nerve. Bradycardia occurs in patients in the later stages of increasing intracranial pressure (ICP) and with cervical spinal cord injuries; it’s usually accompanied by rising systolic blood pressure, widening pulse pressure, and bounding pulse. Tachycardia occurs in patients with acutely increased ICP or a brain injury; it signals decompensation, a condition in which the body has exhausted its compensatory measures for managing ICP, which rapidly leads to death.
BLOOD PRESSURE
Pressor receptors in the medulla continuously monitor blood pressure.
RED FLAG
In a patient with no history of hypertension, rising systolic blood pressure may signal rising ICP. If ICP continues to rise, the patient’s pulse pressure widens as his systolic pressure climbs and diastolic pressure remains stable or falls. In the late stages of acutely elevated ICP, blood pressure plummets as cerebral perfusion fails, resulting in the patient’s death.
Hypotension accompanying a brain injury is also an ominous sign. In addition, cervical spinal cord injuries may interrupt sympathetic nervous system pathways, causing peripheral vasodilation and hypotension.
RESPIRATION
Respiratory centers in the medulla and pons control the rate, depth, and pattern of respiration. Neurologic dysfunction, particularly when it involves the brain stem or both cerebral hemispheres, commonly alters respirations. Assessment of respiration provides valuable information about a CNS lesion’s site and severity. (See Respiratory patterns associated with neurologic impairment, page 30.)
Mental status assessment
The mental status assessment begins when interviewing the patient during the health history. How he responds to your questions gives clues to his orientation and memory and guides the physical assessment as well as the mental assessment. For example, if he complains about confusion or memory problems, you’ll want to concentrate on the mental status part of the examination.
Ask the patient questions that require more than yes-or-no answers. Otherwise, confusion or disorientation might not be immediately apparent. If you have doubts about a patient’s mental status, perform a more detailed screening examination. (See Screening mental status, page 31.)
RESPIRATORY PATTERNS ASSOCIATED WITH NEUROLOGIC IMPAIRMENT
Several patterns displaying impaired respiration due to neurologic dysfunction include:
Cheyne-Stokes respirations — a waxing and waning period of hyperpnea that alternates with a shorter period of apnea, which usually indicates increased intracranial pressure from a deep cerebral or brain stem lesion, or a metabolic disturbance in the brain.
Central neurogenic hyperventilation — a type of hyperpnea that indicates damage to the lower midbrain or upper pons, which may occur as a result of severe head injury.
Apneustic respirations—an irregular breathing pattern characterized by prolonged, gasping inspiration, with a pause at full inspiration followed by expiration; there may also be a pause after expiration, which is an important localizing sign of severe brain stem damage.
Biot’s respirations—late signs of neurologic deterioration, which are rare and may appear abruptly; characterized by irregular and unpredictable rate, rhythm, and depth of respiration, they may reflect increased pressure on the medulla coinciding with brain stem compression.
Respiration impairment—varying degrees can occur due to spinal cord damage above C7, which could weaken or paralyze the respiratory muscles.
The mental status examination consists of checking level of consciousness (LOC), orientation, appearance, behavior, communication, cognitive function, and constructional ability.
LEVEL OF CONSCIOUSNESS
In performing an initial assessment, first evaluate the patient’s LOC.
RED FLAG
A change in the patient’s LOC is the earliest and most sensitive indicator that his neurologic status has altered.
If the patient’s behavior is threatening while performing this initial assessment, he may not be in immediate danger, but as the health care provider, you may be at risk. Therefore, you may need to change the order of the assessment. Always consider the environment and physical condition of the patient. For example, an elderly patient admitted to the health care facility for several days may not be oriented to time, especially if he’s bedridden. Also, consider the patient’s vital signs and need for immediate lifesaving care.
SCREENING MENTAL STATUS
To screen patients for disordered thought processes, ask the questions presented here. An incorrect answer to any question may indicate the need for a complete mental status examination.
QUESTION
FUNCTION SCREENED
What’s your name?
Orientation to person
What’s your mother’s name?
Orientation to other people
What year is it?
Orientation to time
Where are you now?
Orientation to place
How old are you?
Memory
Where were you born?
Remote memory
What did you have for breakfast?
Recent memory
Who’s the U.S. president?
General knowledge
Can you count backward from 20 to 1?
Attention span and calculation skills
Speak the patient’s name in a normal tone of voice and note the response to an auditory stimulus. If he doesn’t respond, use a tactile stimulus, such as touching him gently, squeezing his hand, or shaking his shoulder.
A fully awake patient is alert, open-eyed, and attentive to environmental stimuli. A less-awake patient appears drowsy, has reduced motor activity, and seems less attentive to environmental stimuli. Decreased arousal commonly precedes disorientation.
Use painful stimuli only to assess a patient who’s unconscious or who has a markedly decreased LOC and doesn’t respond to other stimuli. To test response to pain, apply firm pressure over the patient’s nail bed with a blunt, hard object such as a pen. Other acceptable methods include squeezing the trapezius muscle, applying supraorbital pressure, applying mandibular pressure, and performing a sternal rub.
Next, note the type and intensity of stimulus required to elicit a response. Observe if the response is verbally appropriate, if it consists of unintelligible mumbling, body movement or eye opening, or if the patient exhibits no response at all. After you remove the stimulus, observe his level of alertness—for example, if he’s wide awake, drowsy, or drifting to sleep.
After assessing the patient’s level of alertness, compare the findings with results of previous assessments. Note trends, for example, if he’s lethargic more often than usual. Consider factors that could affect patient responsiveness. For example, a normally alert patient may become drowsy after administration of such CNS depressant medications as sedatives and opioids.
Describe a patient’s responsiveness objectively. For example, describe a lethargic patient’s responses this way: “awakened when called loudly, then immediately fell asleep.”
Many terms are used to describe LOC, but their definitions may differ slightly among health care providers. To avoid confusion, clearly describe the patient’s response to various stimuli using these guidelines:
alert—follows commands and responds completely and appropriately to stimuli
lethargic—is drowsy; has delayed responses to verbal stimuli; may drift off to sleep during examination
stuporous—requires vigorous stimulation for a response
comatose—doesn’t respond appropriately to verbal or painful stimuli; can’t follow commands or communicate verbally.
RED FLAG
If the patient has sustained a skull fracture, but appears lucid, and later has a decreased LOC, this could indicate an arterial epidural bleed that requires immediate surgery.
To minimize the subjectivity of LOC assessment and to establish a greater degree of reliability, use the Glasgow Coma Scale. This scale evaluates the patient’s LOC according to three objective behaviors: eye opening, verbal responsiveness (which includes orientation), and motor response. (See Using the Glasgow Coma Scale, pages 34 and 35.)
Several disorders can affect the cerebral hemisphere of the brain stem, and a patient’s LOC may be impaired by any one of them. Such disorders include toxic encephalopathy; hemorrhage; extensive, generalized cortical atrophy; and a tumor or intracranial hemorrhage. Rapid deterioration of LOC, from minutes to hours, usually indicates an acute neurologic disorder requiring immediate intervention. A gradually decreasing LOC, from weeks to months, may reflect a progressive or degenerative neurologic disorder.
ORIENTATION
The orientation portion of the mental status assessment measures the ability of the cerebral cortex to receive and accurately interpret sensory stimuli. It includes three aspects: orientation to person, place, and time. Always ask questions that require the patient to provide more than just a yes-or-no answer. First, find out if the patient is oriented to person by asking his name, and note the response. If the patient is disoriented to person, he may look baffled and may stammer or produce an unintelligible or inaccurate answer. Self-identity usually remains intact until late in decreasing LOC, making disorientation to person an ominous sign.
Next, ask the patient about place. Find out if he can correctly state his location. For example, when looking around the room, note if he concludes that he’s in a health care facility, or if he thinks he’s at home.
A patient in the health care facility disoriented to place most commonly confuses the health care facility’s room with home or some other familiar surrounding; a patient who isn’t in a health care facility, yet is still disoriented to place, such as a patient with Alzheimer’s disease, may fail to recognize familiar home surroundings and may wander off in search of something familiar.
USING THE GLASGOW COMA SCALE
The Glasgow Coma Scale describes a patient’s baseline mental status and helps to detect and interpret changes from baseline findings. When using the Glasgow Coma Scale, test the patient’s ability to respond to verbal, motor, and sensory stimulation, and grade your findings according to the scale. A score of 15 indicates that the patient is alert, can follow simple commands, and is oriented to time, place, and person. A decreased score in one or more categories may signal an impending neurologic crisis. A score of 7 or less indicates severe neurologic damage.
TEST
SCORE
RESPONSE
EYE OPENING RESPONSE
Spontaneously
4
Opens eyes spontaneously
To speech
3
Opens eyes when told to
To pain
2
Opens eyes only to painful stimulus
None
1
Doesn’t open eyes in response to stimuli
MOTOR RESPONSE
Obeys
6
Shows two fingers when asked
Localizes
5
Reaches toward painful stimulus and tries to remove it
Withdraws
4
Moves away from painful stimulus
Abnormal flexion
3
Assumes a decorticate posture (shown below)
Abnormal extension
2
Assumes a decerebrate posture (shown below)
None
1
No response; just lies flaccid (an ominous sign)
VERBAL RESPONSE (TO QUESTION “WHAT YEAR IS THIS?”)
Oriented
5
Tells correct year
Confused
4
Tells incorrect year
Inappropriate words
3
Replies randomly with incorrect words
Incomprehensible
2
Moans or screams
No response
1
No response
TOTAL SCORE
Finally, assess orientation to time by asking the patient to state the year, month, and date. Most people usually answer correctly and can also differentiate day from night if their environment provides enough information; for example, if the room has a window.
RED FLAG
A patient’s orientation to time is usually disrupted first and his orientation to person is disrupted last.
If disorientation to time arises from a physiologic problem, the patient is also likely to mistake unfamiliar surroundings or people for familiar ones. For example, he may confuse the health care facility’s room with his bedroom or mistake a health care provider for a relative. If the disorientation originates from psychiatric disturbances, such as schizophrenia, he may have an unusually bizarre confusion pattern. Answers, such as 1756 or 2054, may indicate a psychiatric disturbance — or a lack of cooperation.
APPEARANCE
Note how the patient behaves, dresses, and grooms himself. Observe his appearance and if he acts appropriately. Note his personal hygiene. If you observe negative findings, such as disheveled or dirty clothing, discuss them with family members to determine whether this is a change. Even subtle changes can signal a new onset of a chronic disease or a more acute change that involves the frontal lobe.
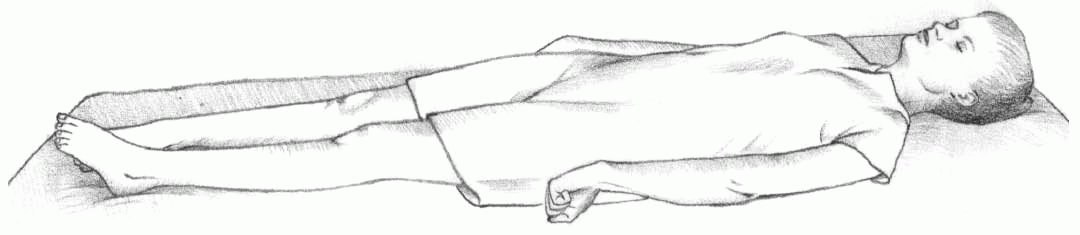
Look at the patient’s color, facial expressions, mobility, deformities, and nutritional state. Observe the patient’s gait, posture, and ability to rise from a chair. Note if he needs assistance to walk, rise from a chair, or get undressed. Observe if he can hear and see you when you’re talking. Observe him for raccoon eyes. Note if he has otorrhea—cerebrospinal fluid leaking from his ears.
RED FLAG
Raccoon eyes could indicate bleeding into the periorbital tissue. Otorrhea could indicate a basilar skull fracture. If the brain stem is lacerated or contused, immediate death can occur. Smaller leakages can resolve in 2 to 10 days.
BEHAVIOR
Assess the patient’s thought content by evaluating the clarity and cohesiveness of his ideas. Observe his conversation for smoothness, with logical transitions between ideas. Note if he has hallucinations, which are sensory perceptions that lack appropriate stimuli; or delusions, which are beliefs not supported by reality. Disordered thought patterns may indicate delirium or psychosis.
Test the patient’s ability to think abstractly by asking him to interpret a common proverb such as “A stitch in time saves nine.” A patient with dementia may interpret a common proverb literally.
Test the patient’s judgment by asking him how he would respond to a hypothetical situation. For example, ask him what he would do if he was in a public building and the fire alarm sounded. Evaluate the appropriateness of his answer.
Throughout the interview, assess the patient’s emotional status. Note his mood, his emotional stability or lability, and the appropriateness of his emotional responses. Also assess his mood by asking how he feels about himself and his future.
AGE AWARE
In elderly patients, symptoms of depression may be atypical—for example, decreased function or increased agitation may occur rather than the usual sad affect.
COMMUNICATION
If the patient’s primary language isn’t English, he may have difficulty communicating. Engage the assistance of family members when English isn’t the patient’s primary language. If the family isn’t available, attempt to contact an interpreter. Use of body language will also be necessary.
Assess the patient’s ability to comprehend speech, writing, numbers, and gestures. Language skills include learning and recalling the parts of the language (such as words), organizing word relationships according to grammatical rules, and structuring message content logically. Speech involves neuromuscular actions of the mouth, tongue, and oropharynx.
Verbal responsiveness
During the interview and physical assessment, observe the patient when you ask a question. If you suspect a decreased LOC, call the patient’s name or gently shake his shoulder to try to elicit a verbal response. Note if he speaks in complete sentences, in phrases, or in single words and if he communicates spontaneously or if he rarely speaks.
Assess the quality of the patient’s speech, such as if it’s unusually loud or soft. Observe the patient for clear articulation, or if his words are difficult to understand. Note the rate and rhythm of his speech.
Note if the patient’s verbal responses are appropriate. Observe him for any difficulty finding or articulating his words. Also, note if he uses made-up words, or neologisms.
If communication problems arise, note if the patient is aware of them. If he appears frustrated or angry when communication fails, note if he continues to attempt to talk, unaware that you don’t comprehend.
If you suspect a language impairment, show the patient a common object, such as a cup or a book, and ask him to name it. Ask the patient to repeat a word that you say, such as dog or breakfast. If the patient appears to have difficulty understanding spoken language, ask him to follow a simple instruction such as “Touch your nose.” If the patient succeeds, then try a two-step command such as “Touch your right knee, then touch your nose.” Keep in mind that language performance tends to fluctuate with the time of day and changes in physical condition. A healthy individual may experience language difficulty when ill or fatigued. Increasing language difficulties may indicate deteriorating neurologic status, warranting further evaluation.
Speech impairment or impaired language function can occur from dysphasia, which is the impaired ability to use or understand language, and aphasia, which is the inability to use or understand language, or both, which indicates injury to the cerebral cortex. Several types of aphasia exist, including:
expressive or Broca’s aphasia—impaired fluency; difficulty finding words; impairment located in the frontal lobe, the anterior speech area
receptive or Wernicke’s aphasia—inability to understand written words or speech; use of made-up words; impairment located in the posterior speech cortex, which involves the temporal and parietal lobes
global aphasia—lack of expressive and receptive language; impairment of both speech areas
facial muscle paralysis—difficulty in articulation and slurred speech
dysarthria—impairment of neuromuscular speech
dysphonia—impairment of voice.
Formal language skills evaluation
The formal language skills evaluation identifies the extent and characteristics of the patient’s language deficits. Usually performed by a speech pathologist, it may help pinpoint the site of a CNS lesion. For example, identifying expressive aphasia, when the patient knows what he wants to say but can’t speak the words, may help diagnose a frontal lobe lesion.
When evaluating the patient, assess these language skills:
Spontaneous speech—show the patient a picture, and ask him to describe what’s going on.
Comprehension—Ask the patient a series of simple yes-or-no questions and evaluate his answers. Use questions with obvious answers. For example: “Does it snow in July?”
Naming—Show the patient various common objects, one at a time, and then ask him to name each one. Typical objects include a comb, ball, cup, and pencil.
Repetition—Ask him to repeat words or phrases such as “no ifs, ands, or buts.”
Vocabulary—Ask the patient to explain the meaning of each of a series of words.
Reading—Ask him to read printed words on cards and perform the action described. For example: “Raise your hand.”
Writing—Ask the patient to write something such as his name and address.
Copying figures—Show the patient several figures, one at a time, and then ask him to copy them. The figures usually become increasingly complex, starting with a circle, an X, and a square and proceeding to a triangle and a star.
COGNITIVE FUNCTION
Assessing cognitive function involves testing the patient’s memory, orientation, attention span, calculation ability, thought content, abstract thinking, judgment, insight, and emotional status.
To test your patient’s orientation, memory, and attention span, use the mental status screening questions discussed previously. Always consider the patient’s environment and physical condition when assessing orientation. Also, when the person is intubated and can’t speak, ask questions that require only a nod, such as “Do you know you’re in the hospital?” and “Are we in Pennsylvania?” The patient with an intact short-term memory can generally repeat five to seven nonconsecutive numbers right away and again 10 minutes later.
RED FLAG
Short-term memory is commonly affected first in the patient with a neurologic disease.
When testing attention span and calculation skills, keep in mind that lack of mathematical ability and anxiety can affect the patient’s performance. If he has difficulty with numeric computation, ask him to spell the word “world” backward. While he’s performing these functions, note his ability to pay attention.
CONSTRUCTIONAL ABILITY
The patient’s ability to perform simple tasks and use various objects reflects constructional ability. Apraxia and agnosia are two types of constructional disorders.
Apraxia is the inability to perform purposeful movements and make proper use of objects and is commonly associated with parietal lobe dysfunction. It can appear in any of four types. Ideomotor apraxia is the inability to understand the effect of motor activity; the ability to perform simple activities, but without awareness of performing them; and the inability to perform actions on command. Ideational apraxia is the awareness of actions that need to be done accompanied by an inability to perform them. Constructional apraxia is the inability to copy a design, such as a square or the face of a clock. Finally, dressing apraxia is the inability to understand the meaning of various articles of clothing or the sequence of actions required to get dressed.
Agnosia is the inability to identify common objects and may indicate a lesion in the sensory cortex. Agnosia types include visual, which is the inability to identify common objects unless they’re touched; auditory, the inability to identify common sounds; and body image, the inability to identify body parts by sight or touch, the inability to localize a stimulus, or denial of existence of half of the body.
Cranial nerve assessment
There are 12 pairs of cranial nerves (CNs). These nerves transmit motor or sensory messages, or both, primarily between the brain and brain stem and the head and neck. Cranial nerve assessment provides valuable information about the condition of the CNS, particularly the brain stem.
OLFACTORY (CN I)
To assess the olfactory nerve, first check the patency of both nostrils, then instruct the patient to close his eyes. Occlude one nostril and hold a familiar, pungent-smelling substance— such as coffee, lemon, soap, or peppermint—under his nose and ask its identity. Repeat this technique with the other nostril.
If the patient reports detecting the smell but can’t name it, offer a choice such as “Do you smell lemon, coffee, or peppermint?” The patient should be able to detect and identify the smell correctly. The location of the olfactory nerve makes it especially vulnerable to damage from facial fractures and head injuries.
Damage to CN I may be due to disorders of the base of the frontal lobe, such as tumors or arteriosclerotic changes.
RED FLAG
The sense of smell remains intact as long as one of the two olfactory nerves exists; it’s permanently lost (anosmia) if both nerves are affected. Anosmia may also result from nonneurologic causes, such as nasal congestion, sinus infection, smoking, and cocaine use. Once anosmia is present, it can also impair the sense of taste. Therefore, a complaint about food taste may signal CN I damage.
OPTIC (CN II) AND OCULOMOTOR (CN III)
To assess the optic nerve, check visual acuity, visual fields, and the retinal structures. To assess the oculomotor nerve, check pupil size, pupil shape, and pupillary response to light.
To test visual acuity and retinal structure quickly and informally, have the patient read a newspaper, starting with large headlines and moving to small print.
DETECTING VISUAL FIELD DEFECTS
Here are some examples of visual field defects. The black areas represent vision loss.
LEFT
RIGHT
1. Blindness of right eye
2. Bitemporal hemianopsia, or loss of half the visual field
3. Left homonymous hemianopsia
4. Left homonymous hemianopsia, superior quadrant
Test visual fields with a technique called confrontation. To do this, stand 2′ (0.6 m) in front of the patient, and have him cover one eye. Then close one of your eyes and bring your moving fingers into the patient’s visual field from the periphery. Ask him to tell you when he sees your hand. Test each quadrant of the patient’s visual field, and compare his results with your own. Chart any defects you find. (See Detecting visual field defects.)
A visual field defect may signal a stroke, head injury, or brain tumor. The area and extent of the loss depend on the lesion’s location.
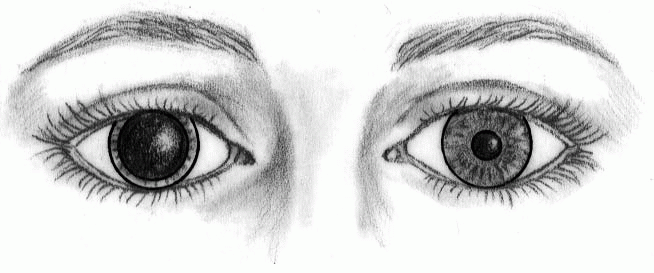
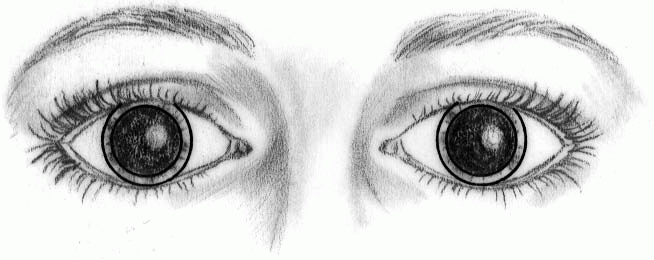
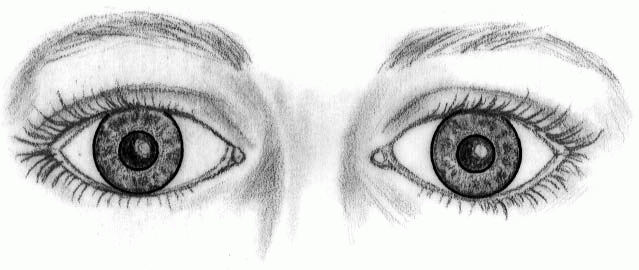
When assessing pupil size, look for trends. For example, watch for a gradual increase in the size of one pupil or the appearance of unequal pupils in a patient whose pupils were previously equal. The pupils should be equal, round, and reactive to light.
RED FLAG
In a blind patient with a nonfunctional optic nerve, light stimulation will fail to produce either a direct or a consensual pupillary response. However, a legally blind patient may have some optic nerve function, which causes the blind eye to respond to direct light. In a patient who’s totally blind in only one eye, the pupil of the eye with the intact optic nerve will react to direct light stimulation, whereas the blind eye, because it receives sensory messages from the functional optic nerve, will respond consensually.
Pupil size can be affected by increased ICP, which causes a change in responsiveness or pupil size on the affected side, resulting in dilation of the pupil ipsilateral to the mass lesion; as ICP rises, the other oculomotor nerve becomes affected, causing both pupils to become oval or react sluggishly to light shortly before dilating. Without treatment, both pupils become fixed and dilated. The hippus phenomenon causes brisk pupil constriction in response to light followed by a pulsating dilation and constriction, which may be normal in some patients but may also reflect early oculomotor nerve compression. Optic and oculomotor nerve damage may also affect pupil size by impairing the pupillary response to light, which indicates neurologic demise. Lastly, anisocoria, or unequal pupils, which are normal in about 20% of people, occurs when pupil size doesn’t change with the amount of illumination. (See Understanding pupillary changes, page 44.)
OCULOMOTOR (CN III), TROCHLEAR (CN IV), AND ABDUCENS (CN VI)
To test the coordinated function of the oculomotor, trochlear, and abducens nerves, assess them simultaneously by evaluating the patient’s extraocular eye movement. (See Testing extraocular muscles, page 45.) The patient’s eyes should move smoothly and in a coordinated manner through all six directions of eye movement including left superior, left lateral, left inferior, right superior, right lateral, and right inferior.
Observe each eye for rapid oscillation, known as nystagmus; movement not in unison with that of the other eye, called disconjugate movement; or inability to move in certain directions, known as ophthalmoplegia. Also note any complaint of double vision, or diplopia. Nystagmus may indicate a disorder of the brain stem, the cerebellum, or the vestibular portion of CN VIII. It may also imply drug toxicity such as from the anticonvulsant, phenytoin.
UNDERSTANDING PUPILLARY CHANGES
Use this chart as a guide when observing your patient for pupillary changes.
PUPILLARY CHANGE
POSSIBLE CAUSES
Unilateral, dilated (4 mm), fixed, and nonreactive
Uncal herniation with oculomotor nerve damage
Brain stem compression
Increased intracranial pressure
Tentorial herniation
Head trauma with subdural or epidural hematoma
May be normal in some people
Bilateral, dilated (4 mm), fixed, and nonreactive
Severe midbrain damage
Cardiopulmonary arrest (hypoxia)
Anticholinergic poisoning
Bilateral, midsize (2 mm), fixed, and nonreactive
Midbrain involvement caused by edema, hemorrhage, infarctions, lacerations, contusions
Bilateral, pinpoint (<1 mm), and usually nonreactive
Lesions of pons, usually after hemorrhage
Unilateral, small (1.5 mm), and nonreactive
Disruption of sympathetic nerve supply to the head caused by spinal cord lesion above T1
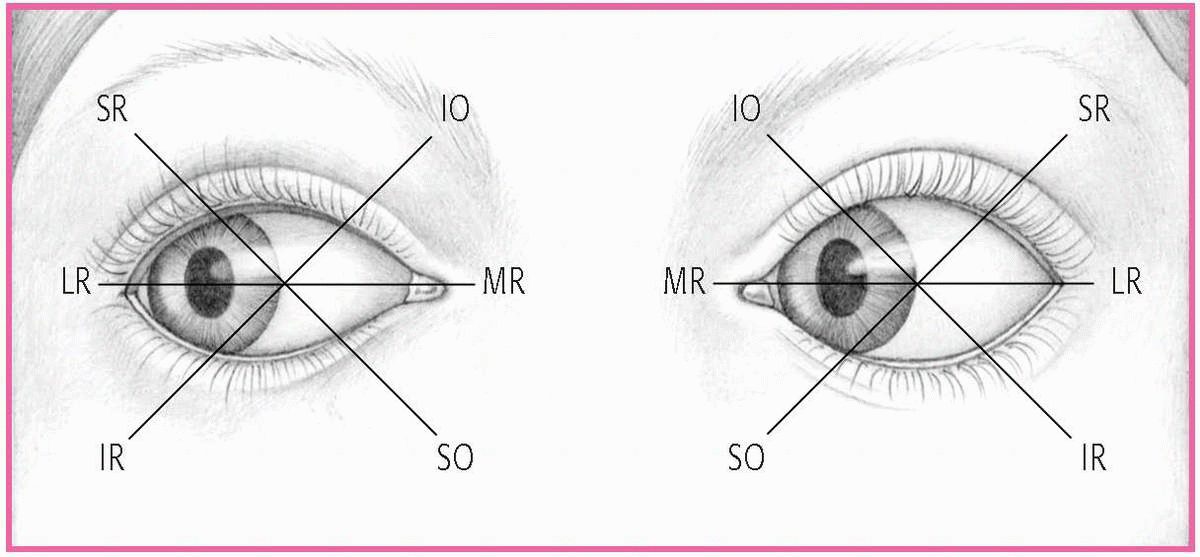
TESTING EXTRAOCULAR MUSCLES
The coordinated action of six muscles controls eyeball movements. To test the function of each muscle and the cranial nerve (CN) that innervates it, ask the patient to look in the direction controlled by that muscle. The six directions you can test make up the cardinal fields of gaze. The patient’s inability to turn the eye in the designated direction indicates muscle weakness or paralysis.
SR-superior rectus (CN III)
IO-inferior oblique (CN III)
LR-lateral rectus (CN VI)
MR-medial rectus (CN III)
IR-inferior rectus (CN III)
SO-superior oblique (CN IV)
RED FLAG
Increased ICP can put pressure on CN IV, causing impaired extraocular eye movement inferiorly and medially, and CN VI, causing impaired extraocular eye movement laterally.
The oculomotor nerve is also responsible for eyelid elevation and pupillary constriction. Drooping of the patient’s eyelid, or ptosis, can result from a defect in the oculomotor nerve. To assess ptosis more accurately, have the patient sit upright.
TRIGEMINAL (CN V)
To assess the sensory portion of the trigeminal nerve, gently touch the right side and the left side of the patient’s forehead with a cotton ball while his eyes are closed. Instruct him to state the moment the cotton touches the area. Compare his response on both sides. Repeat the technique on the right and left cheek and on the right and left jaw. Next, repeat the entire procedure using a sharp object. The cap of a disposable ballpoint pen can be used to test light touch with the dull end and sharp stimuli with the sharp end. If an abnormality appears, test for temperature sensation by touching the patient’s skin with test tubes filled with hot and cold water and asking the patient to differentiate between them. The patient should report feeling both light touch and sharp stimuli in all three tested areas.
Peripheral nerve damage can create a loss of sensation in any or all three regions supplied by the trigeminal nerve. Trigeminal neuralgia causes severe, piercing, or stabbing pain over one or more of the facial dermatomes. A lesion in the cervical spinal cord or brain stem can produce impaired sensory function in each of the three areas.
To assess the motor portion of the trigeminal nerve, ask the patient to clench his jaws. Palpate the temporal and masseter muscles bilaterally, checking for symmetry. Try to open his clenched jaws. Next, watch the patient while he’s opening and closing his mouth for asymmetry. The jaws should clench symmetrically and remain closed against resistance.
A lesion in the cervical spinal cord or brain stem can produce impaired motor function in regions supplied by the trigeminal nerve, weakening the patient’s jaw muscles, causing the jaw to deviate toward the affected side when chewing, and allowing residual food to collect in the affected cheek.
To assess the patient’s corneal reflex, stroke a wisp of cotton lightly across a cornea. The lids of both eyes should close. (See Eliciting the corneal reflex.) An absent corneal reflex may result from peripheral nerve or brain stem damage. However, a diminished corneal reflex commonly occurs in patients who wear contact lenses.
ELICITING THE CORNEAL REFLEX
To elicit the corneal reflex, have the patient turn her eyes away from you to avoid involuntary blinking during the procedure. Then approach the patient from the opposite side, out of her line of vision, and brush the cornea lightly with a fine wisp of sterile cotton. Repeat the procedure on the other eye. The lids of both eyes should close.
Only gold members can continue reading. Log In or Register to continue