Asymmetric Cerebral Hemispheres
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
Normal Variant
Encephalomalacia, General
Post-Ischemic Encephalomalacia
Post-Traumatic Encephalomalacia
Post-Inflammatory Encephalomalacia
Contusion/Traumatic Cerebral Edema
Cerebral Ischemia-Infarction, Acute
Cerebral Infarction, Chronic
Alzheimer Dementia
Multi-Infarct Dementia
CMV, Congenital
Frontotemporal Dementia
Dyke-Davidoff-Masson
Less Common
Hypoxic Ischemic Encephalopathy
Encephalitis
Sturge-Weber Syndrome
Plagiocephaly
MELAS
Hemimegalencephaly of Tuberous Sclerosis
Rare but Important
Hemimegalencephaly (Sporadic or Familial)
Pachygyria-Polymicrogyria
Gliomatosis Cerebri
Epidermal Nevus Syndrome
Schizencephaly
Encephalocraniocutaneous Lipomatosis
Proteus Syndrome
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Differential diagnosis list is vast and could logically be subdivided as follows
One hemisphere larger than the other
One hemisphere smaller than the other
Helpful Clues for Common Diagnoses
Normal Variant
Minor asymmetry of otherwise normal appearing density/intensity parenchyma
Substantial individual diversity of left-right gyral cerebral cortex asymmetries
Cerebral asymmetry patterns are not universal & show variation based on origin
Encephalomalacia, General
All etiologies appear as CSF replacing destroyed parenchyma due to
Post-ischemic loss of tissue following parenchymal hypoxic cell death
Post-traumatic loss from parenchymal irreversible traumatic insult
Post-inflammatory loss by irreversibly injured tissue
Post-Traumatic Encephalomalacia
Parenchymal loss replaced by CSF
Occur in characteristic locations where brain is adjacent to bony protuberance or dural fold
Contusion/Traumatic Cerebral Edema
Patchy superficial hemorrhages within edematous background, loss of gray-white distinction
Swelling with loss of sulci, fissures, & cisterns
Cerebral Ischemia-Infarction, Acute
Early cortical swelling in defined vascular distribution(s)
DWI restriction with correlating ADC map
Cerebral Infarction, Chronic
Volume loss with gliosis along margins
Loss in a defined vascular distribution
Alzheimer Dementia
Parietal & temporal cortical atrophy with disproportionate hippocampal volume loss
Often affects brain asymmetrically
Multi-Infarct Dementia
Multifocal infarcts of gray matter, white matter, basal ganglia, pons
Usually bilateral, but may be unilateral
CMV, Congenital
Microcephaly, cerebral calcification, cortical gyral abnormalities, cerebellar hypoplasia, & myelin delay or destruction
Gestational age at time of infection determines pattern of CNS injury
Frontotemporal Dementia
Caused by focal cortical atrophy involving frontal &/or temporal lobes
Worse atrophy of dominant hemisphere
Dyke-Davidoff-Masson
Cerebral hemiatrophy with ipsilateral hypertrophy of the skull and sinuses
Caused by an intrauterine or perinatal carotid artery infarction
Helpful Clues for Less Common Diagnoses
Hypoxic Ischemic Encephalopathy
Acquired neonatal condition generally attributed to cerebral hypoperfusion
Several brain injury patterns attributed to differing clinical variables
Encephalitis
Abnormal T2 hyperintensity of gray matter ± white matter, or deep gray nuclei
Diffuse brain parenchymal inflammation caused by a variety of pathogens, most commonly viruses
Sturge-Weber Syndrome
Cortical Ca++, atrophy, and enlarged ipsilateral choroid plexus
Unilateral 80%, bilateral 20%; occipital > parietal > frontal/temporal lobes > diencephalon/midbrain > cerebellum
Plagiocephaly
CT: Osseous asymmetry with thickened & sclerotic suture margins
Premature unilateral closure of coronal &/or lambdoidal sutures
MELAS
Stroke-like cortical lesions crossing typical vascular territories
Acute → gyriform swelling; chronic → atrophy
Hemimegalencephaly of Tuberous Sclerosis
Unilateral lobar/hemispheric overgrowth
Look for other markers of TSC (e.g., subependymal nodules)
Helpful Clues for Rare Diagnoses
Hemimegalencephaly (Sporadic or Familial)
Hamartomatous overgrowth of hemisphere
Defect of cellular organization, neuronal migration
Pachygyria-Polymicrogyria
Findings range from incomplete lissencephaly to excessively small & prominent gyral convolutions
Disorder of neuronal migration
Gliomatosis Cerebri
T2 hyperintense infiltrating mass with enlargement of involved hemisphere
Typically hemispheric white matter involvement, involves cortex in 19%
Epidermal Nevus Syndrome
Hemimegalencephaly is most common CNS abnormality
Also migration abnormalities, vascular malformations, corpus callosal agenesis, Dandy-Walker, myelomeningocele, Chiari malformations, & tumors
Schizencephaly
Transmantle gray matter lined clefts
“Closed-lip” (small) or “open-lip” (large)
Encephalocraniocutaneous Lipomatosis
Hemispheric atrophy, ventriculomegaly with ipsilateral alopecia overlying a scalp lipoma
Hydrocephalus is frequently present
Proteus Syndrome
Complex hamartomatous disorder involving half the body
CNS: Hemimegalencephaly, subependymal calcified nodules, & periventricular cysts
Image Gallery
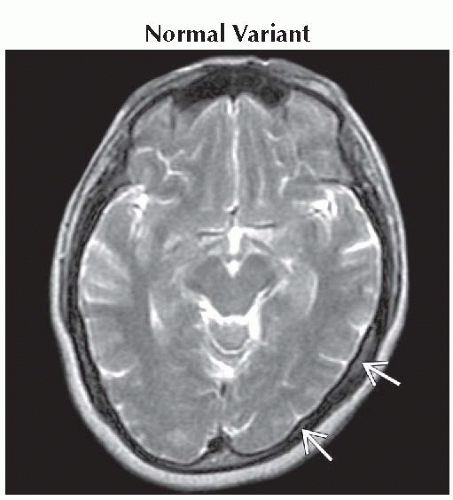 Axial T2WI MR shows normal asymmetry, especially involving the left temporal/occipital lobes  as compared to the right, in this patient with headache and a normal MR. as compared to the right, in this patient with headache and a normal MR. |
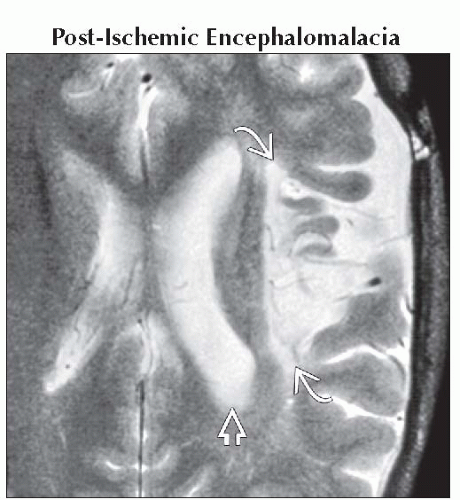 Axial T2WI MR shows typical MCA distribution chronic infarct as encephalomalacia with gliotic hyperintense margins  . Adjacent sulci & ventricle . Adjacent sulci & ventricle  are prominent from volume loss. are prominent from volume loss. |
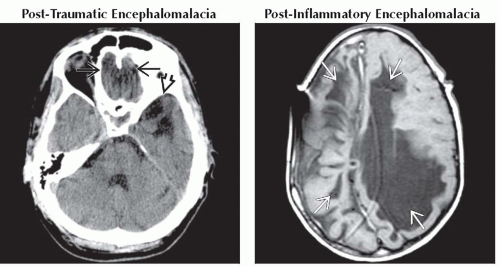 (Left) Axial NECT demonstrates post-traumatic encephalomalacia of bilateral rectus gyri
 & left temporal tip & left temporal tip  in characteristic locations adjacent to bony surfaces. (Right) Axial T1 C+ MR shows extensive cavitation of bilateral hemispheric white matter in characteristic locations adjacent to bony surfaces. (Right) Axial T1 C+ MR shows extensive cavitation of bilateral hemispheric white matter  with extreme volume loss and cavity retraction bilaterally, right more than left, all sequelae from Citrobacter meningitis. with extreme volume loss and cavity retraction bilaterally, right more than left, all sequelae from Citrobacter meningitis.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|