Asymmetric Lateral Ventricles
Bronwyn E. Hamilton, MD
DIFFERENTIAL DIAGNOSIS
Common
Normal Variant
Extrinsic Mass Effect
Encephalomalacia, General
Intraventricular Hemorrhage
Herniation Syndromes, Intracranial
Surgical Defects
Obstructive Hydrocephalus
Choroid Plexus Cyst
Less Common
Ventriculitis
CSF Shunts and Complications
Meningioma
Choroid Plexus Papilloma
Neurocysticercosis
Rare but Important
Intraventricular Synechiae/Adhesions
Choroid Plexus Carcinoma
Ependymal Cyst
Dyke-Davidoff-Masson
Hemimegalencephaly
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Asymmetric lateral ventricles are most commonly seen as a normal variant
Helpful Clues for Common Diagnoses
Normal Variant
Asymmetric lateral ventricles seen in 5-10% of normal population
Asymmetry mild-moderate, left > right
Septum may be displaced across the midline
No associated mass effect, herniation, or parenchymal atrophy
Must exclude underlying mass or obstructing lesion
Extrinsic Mass Effect
Etiologies include mass, hemorrhage, infarct, infection
Mass can cause ventricular deformity, subfalcine herniation
Encephalomalacia, General
Parenchymal loss results in compensatory ventricular enlargement
Common etiologies include chronic infarct, trauma, surgery
Intraventricular Hemorrhage
Involved ventricle may dilate early from mass effect
Chronic dilation may be due to scarring from adhesions
Etiologies include trauma, AVM, basal ganglia hemorrhage
Herniation Syndromes, Intracranial
Subfalcine herniation: Cingulate gyrus herniates under falx
Ipsilateral lateral ventricle compressed
Foramen of Monro obstructs, causes contralateral lateral ventricle enlargement
Unilateral descending transtentorial herniation (uncal): Herniation of medial temporal lobe inferiorly
Contralateral temporal horn becomes entrapped & enlarges
Entrapped ventricle: Typically temporal horn, by extrinsic mass effect
Surgical Defects
Look for calvarial defect or “tract”
Typically related to resection of mass
Ventricle enlarged unilateral to defect
Obstructive Hydrocephalus
Typically acquired & bilateral
May be unilateral if shunt complication or obstructing tumor is cause
Rare: Colloid cyst may obstruct unilateral foramen of Monro & cause unilateral ventriculomegaly
Choroid Plexus Cyst
Nonneoplastic, noninflammatory cyst of the choroid plexus
Common incidental finding in older patients (40% prevalence)
Typically bilateral, may be unilateral & enlarge lateral ventricle
Helpful Clues for Less Common Diagnoses
Ventriculitis
Ventriculomegaly with debris level, enhancing ependyma
May affect lateral ventricles asymmetrically, particularly if related to shunt placement or abscess rupture
CSF Shunts and Complications
Common complications include shunt obstruction or breakage, infection, overdrainage
Asymmetric ventricles may result from overdrainage or underdrainage of an “isolated” ventricle
Meningioma
Intraventricular meningioma rare, typically left lateral ventricle
Associated with choroid plexus
Smooth enhancing intraventricular mass
Choroid Plexus Papilloma
Enhancing, lobulated intraventricular mass in a child
50% in lateral ventricle atrium, left > right
May obstruct CSF flow or overproduce CSF
May have CSF spread of tumor
Neurocysticercosis
Intraventricular disease uncommon
Rarely may obstruct unilateral foramen of Monro & cause asymmetric lateral ventricle
Cyst with “dot” representing scolex characteristic
T1 & FLAIR best show intraventricular cysts
Helpful Clues for Rare Diagnoses
Intraventricular Synechiae/Adhesions
May be congenital or acquired (prior bleed, infection, tumor)
Look for enhancing septae, intraventricular cysts within ventricle
Choroid Plexus Carcinoma
Enhancing intraventricular mass & ependymal invasion in young child
CSF seeding common
Ependymal Cyst
Nonenhancing thin-walled cyst with CSF density/intensity
Lateral ventricle most common location
Dyke-Davidoff-Masson
Antenatal unilateral hemispheric infarction causes cerebral hemiatrophy
Ipsilateral calvarial thickening & hyperpneumatized frontal sinuses, temporal bones
Dilated ventricle from volume loss is ipsilateral to small hemisphere
Hemimegalencephaly
Unilateral hemispheric enlargement
Dilated, usually dysmorphic ventricle ipsilateral to enlarged hemisphere
Ipsilateral extracalvarial soft tissues may be larger
Other Essential Information
High resolution “MR cisternography”: CISS, balanced FFE, FIESTA
May detect small septations or arachnoid membranes causing obstruction
Cine CSF flow study may help detect physiologic flow obstruction from arachnoid webs or membranes
May assess adequacy of drainage procedures
Image Gallery
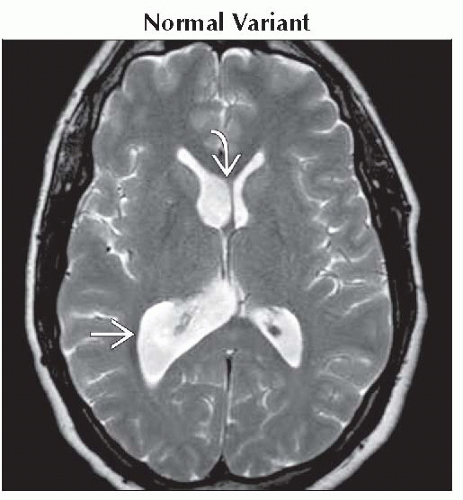 Axial T2WI MR shows asymmetrically large right ventricular system
 representing a normal variant. Note mild displacement of the septum pellucidum across midline representing a normal variant. Note mild displacement of the septum pellucidum across midline  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|