Detection
In-vitro detection of autoantibodies is based on visualization of the binding reaction between the autoantibody and its target antigen. Standard immunological methods include the indirect immunofluorescence test (IFT), ELISA, immunoblot, radioreceptor assay (RRA), and immunoprecipitation assays (Chap. 4, “Methods of Immune Complex Analysis”).
For diagnostic purposes, it is the detection of autoantibodies in the serum that is important; only exceptionally does their detection in the CSF yield meaningful additional information.
Suitable methods for demonstrating and differentiating between the various gammopathies and cryoglobulinemias include serum protein electrophoresis and (as immunoprecipitation assays) immunoelectrophoresis and immunofixation electrophoresis (Chap. 4, “Methods of Immune Complex Analysis”).
Indirect immunofluorescence test (IFT). This test serves as a screening method for a broad panel of autoantibodies including antinuclear antibody (ANA) and anti-neutrophil cytoplasmic antibody (ANCA). It is also a screening test for detecting antibodies to skeletal muscle proteins (titin, ryanodine receptor) in patients with myasthenia gravis and aquaporin-4 (AQP4) antibodies in patients with neuromyelitis optica spectrum disorders.
ELISA. ELISA is used for detecting the fine specificities of ANA and ANCA, phospholipid antibodies, antibodies against ribosomal P proteins, IgM rheumatoid factors and α-fodrin, and also myositis-associated antibodies, skeletal muscle antibodies, and ganglioside antibodies.
Immunoblot. Immunoblots are used for detecting the fine specificities of ANA, antibodies against ribosomal P proteins, α-fodrin antibodies, myositis-associated antibodies, and ganglioside antibodies. Preparations of CNS myelin are used for detecting antibodies to myelin-associated glycoprotein (MAG) in the immunoblot.
Radioreceptor assay (RRA). Radioreceptor assay is the standard method for detecting antibodies to acetylcholine receptors (AchR) and antibodies against various ion channels. For the purpose of detecting AchR antibodies, purified 125I-bungarotoxin-labeled AchR from human skeletal muscles are used. Antibodies against voltage-dependent calcium and potassium channels are detected by using prepurified P/Q subtype calcium or potassium channel proteins labeled with 125I-ω-conotoxin MVIIC or 125I-α-dendrotoxin.
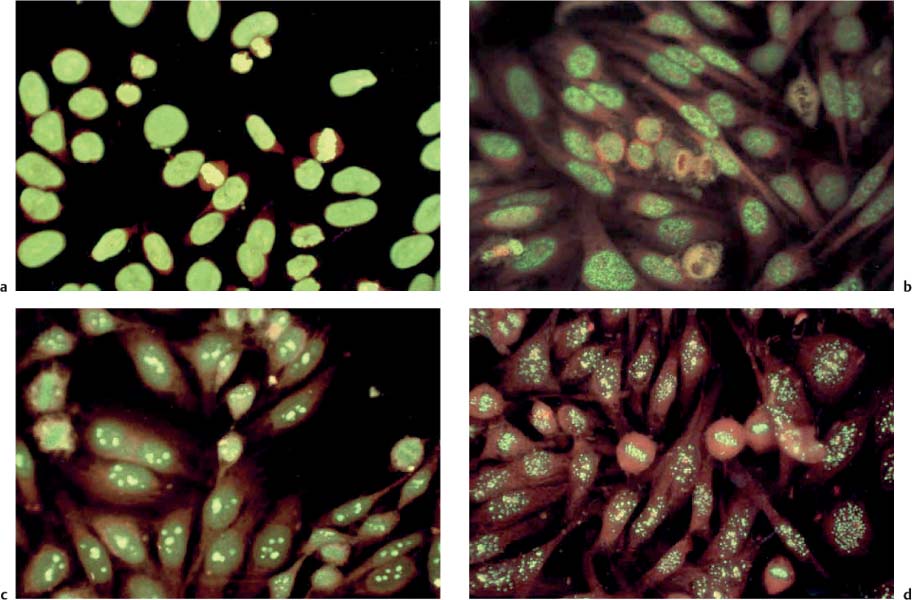
Fig. 7.1 a–d ANA patterns on HEp-2 cells in the indirect immunofluorescence test.
a Homogeneous pattern.
b Fine-granular (spotted) pattern.
c Nucleolar pattern.
d Centromeric pattern.
Thin-layer chromatography (TLC). In addition to ELISA and immunoblot, the TLC overlay technique is suitable for detecting ganglioside antibodies in the test serum. This method is available only in specialized laboratories.
Immunoprecipitation. Immunodiffusion and countercurrent electrophoresis are used for detecting myositis-associated antibodies. Immunoelectrophoresis and—even more sensitive—immunofixation electrophoresis are used to determine the class of immunoglobulin and the associated type of monoclonal free light chains (Bence Jones proteins, BJP). Immunofixation electrophoresis is also used to differentiate the cryoprecipitates in cryoglobulinemia (types I–III, see Chap. 10, “Guillain-Barré Syndrome and Other Immune-Mediated Neuropathies”), using monovalent or polyvalent immunoglobulin class-specific antisera. Immunonephelometry is indicated for quantitative determination of rheumatoid factors.
Examples
Antinuclear Antibodies (ANA)
Definition of ANA
ANA include a diversity of antibody subspecificities directed against distinct nuclear structures. They are characteristically used in laboratory diagnostic tests for connective tissue diseases.
ANA analysis. The standard screening method for detecting ANA is the IFT. Special microscopic slides for ANA detection are commercially available, with human epidermoid carcinoma cells (HEp-2) as a substrate on their test fields. To optimize sensitivity and specificity, some test systems also contain frozen sections of primate liver. Comparison of the fluorescence patterns (homogeneous, granular/spotted, nucleolar, centromeric, and peripheral) in HEp-2 cells and liver sections allows an initial differentiation of ANA subspecificities. Figure 7.1 shows examples of autoantibodies detected by this method:
• Antibodies against double-stranded DNA (anti-dsDNA) and histones yield homogeneous immunofluorescence.
• Antibodies against Sjögren’s syndrome antigens A and B (anti-SS-A, anti-SS-B) yield a fine-granular immunofluorescence.
• Antibodies against polymyositis–scleroderma (anti-PMScl) yield a nucleolar staining pattern.
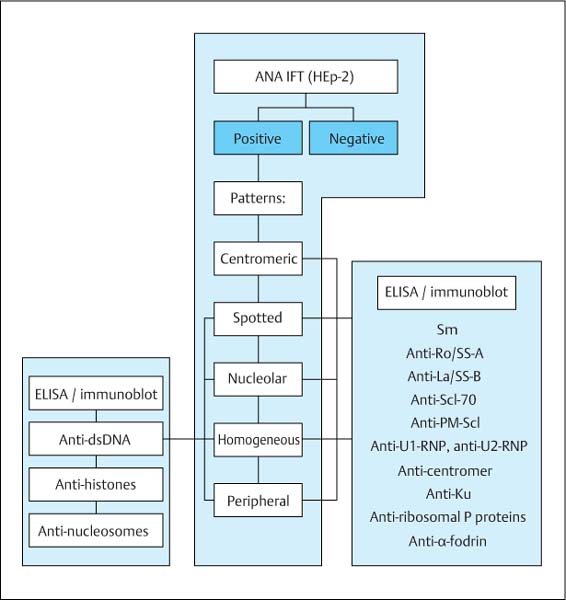
Fig. 7.2 Flow chart of ANA analysis. The fluorescence patterns in the indirect immunofluorescence test (IFT) allow initial differentiation of ANA subspecificities. Fine specificities are subsequently identified by ELISA or immunoblot.
Reference range:
 In most laboratories, titers of 1:80 to 1:160 are considered positive.
In most laboratories, titers of 1:80 to 1:160 are considered positive.
 Titers of 1:40 to 1:80 are considered borderline.
Titers of 1:40 to 1:80 are considered borderline.
For reasons of cost, ANA analysis should be carried out one step at a time (Fig. 7.2).
ANA follow-up analysis. Depending on the suspected clinical diagnosis, a positive ANA immunofluorescence test is followed by fine differentiation of ANA specificity. The commercially available immunoblot or ELISA systems for this purpose use defined purified or, less often, recombinant nuclear target antigens as substrates. It is only by ANA follow-up analysis that a nosologic classification of the associated rheumatoid syndrome is made possible (see Chap. 10, “Systemic Vasculitis and Connective Tissue Diseases”). The now outdated term “extractable nuclear antigen” (ENA) refers in the widest sense to all autoantibodies detectable using nuclear extract preparations. It should no longer be used as a generic term for ANA follow-up analysis.
Reference ranges for ANA subspecificities:
 usually vary among the suppliers of the test kits.
usually vary among the suppliers of the test kits.
Anti-neutrophil Cytoplasmic Antibodies (ANCA)
Definition of ANCA
ANCA are specific for enzymes localized in the granules of neutrophil granulocytes. They are characteristically used in laboratory diagnostic tests for systemic immune vasculitis.
Immunofluorescence test. The screening test for ANCA is the IFT. ANCAs are detected using commercially available microscopic slides with ethanol-fixed neutrophil granulocytes as a substrate on their test fields. In some test systems they also contain frozen sections of primate liver in order to differentiate between ANCA and ANA. Three fluorescent patterns can be distinguished in this test:
• Cytoplasmic ANCAs (cANCAs) are characterized by finegranular cytoplasmic immunofluorescence with central accentuation (Fig. 7.3 a). The specific target antigen of the cANCA subtype is proteinase 3 (anti-PR3/cANCA), an enzyme of the principal granules of myeloid cells and granulocytes, and of the lysosomes of monocytes. Anti-PR3/cANCA occur primarily in Wegener’s disease and in a subgroup of patients with Churg-Strauss syndrome (allergic granulomatosis) (see Chap. 10, “Systemic Vasculitis and Connective Tissue Diseases”).
• Perinuclear ANCAs (pANCAs) are characterized by a sharply delimited perinuclear immunofluorescence, and their primary target antigen is myeloperoxidase (anti-MPO/pANCA), an enzyme localized in the azurophil granules of granulocytes (Fig. 7.3 b). Anti-MPO/pANCA occurs predominantly in microscopic polyangiitis and, like anti-PR3/cANCA, in a subgroup of patients with Churg-Strauss syndrome.
• Atypical ANCAs (aANCAs; not relevant for diagnosis of neurological diseases) are characterized by an atypical pattern with homogeneous cytoplasmic immunofluorescence and additional staining of the perinuclear zone. They are found in chronic inflammatory intestinal diseases and primary sclerosing cholangitis. Their target antigens are not known.
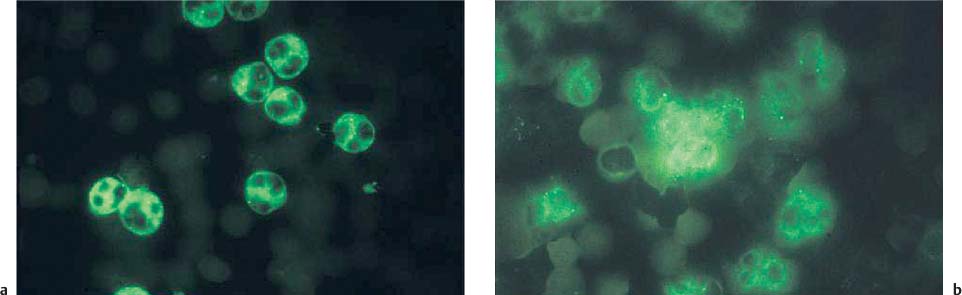
Fig. 7.3 a, b ANCA immunofluorescence patterns.
a Anti-PR3/cANCA on neutrophil granulocytes in the indirect immunofluorescence test yields a fine-granular cytoplasmic pattern.
b Anti-MPO/pANCA on neutrophil granulocytes in the indirect immunofluorescence test yields a perinuclear pattern with or without exclusion of the nucleus.
ELISA. Quantitative determination and fine differentiation of cANCA and pANCA is done with ELISA using total extracts or purified target antigens.
Preanalytical requirements. If stored for more than 72 hours, serum should be kept at −20°C or, even better, at −70°C.
Reference range:
 Titers of 1:10 or higher are generally considered positive.
Titers of 1:10 or higher are generally considered positive.
Phospholipid Antibodies
Definition of Phospholipid Antibodies
These are found in connective tissue diseases or in primary antiphospholipid syndrome (APS) and include antibodies of various fine specificities, which are identified using various methods of detection. They are directed against negatively charged phospholipids and cause false-positive results in pathogen-specific syphilis screening reactions (venereal disease research laboratory test, VDRL; cardiolipin complement fixation test, CCF) as well as lupus anticoagulant phenomena with prolonged activated partial thromboplastin time (aPTT).
Cardiolipin. Antibodies to cardiolipin can be detected by ELISA in the presence of β2-glycoprotein I as a cofactor.
Reference ranges:
 Cardiolipin IgM: 8–14 MPL-U/mL (< 8 definitely negative; > 14 definitely positive).
Cardiolipin IgM: 8–14 MPL-U/mL (< 8 definitely negative; > 14 definitely positive).
 Cardiolipin IgG: 15–22 GPL-U/mL (< 15 definitely negative; > 22 definitely positive).
Cardiolipin IgG: 15–22 GPL-U/mL (< 15 definitely negative; > 22 definitely positive).
Lupus anticoagulant. This term refers to antibodies that bind to phospholipid protein complexes on the cell membrane and interfere with blood clotting. In the presence of lupus anticoagulant, the clotting time in a phospholipiddependent coagulation test is unusually prolonged. The test material is citrate plasma, and the method of determination is aPTT. Paradoxically, lupus anticoagulant increases the risk of thrombosis.
Reference ranges:
 26–36 seconds, depending on the reagent used.
26–36 seconds, depending on the reagent used.
Paraproteins
Definition of Paraproteins
Paraproteins are monoclonal immunoglobulins that are generated by uncontrolled proliferation of a single B cell clone.
There are two types of paraproteins associated with neuropathy (see Chap. 10, “Paraneoplastic Neurological Syndromes”):
• Isolated paraproteins (monoclonal gammopathy of undetermined significance, MGUS).
• Paraproteins accompanying hematologic neoplasia (multiple myeloma, Waldenström’s macroglobulinemia).
The monoclonal immunoglobulin may:
• Be complete (e. g., IgG-κ, IgA-λ).
• Consist of free light chains of one type only (e. g., κ or λ, also known as Bence Jones protein, BJP).
• Be combined of the intact protein and BJP.
• Be composed of free heavy chains only (e. g., α-, γ-, μ-chains).
• Be composed of several clonal immunoglobulins.
Analysis. Paraproteins appear as sharp peaks (M spike, M protein) in the exploratory electrophoresis of serum and urine proteins. For confirmation and typing of monoclonal gammopathy, immunoelectrophoresis and immunofixation electrophoresis are used.
Detection sensitivity for monoclonal immunoglobulin production:
 Serum electrophoresis: < 2 g/L.
Serum electrophoresis: < 2 g/L.
 Immunoelectrophoresis: 1–2 g/L.
Immunoelectrophoresis: 1–2 g/L.
 Immunofixation electrophoresis: 20–30 mg/L.
Immunofixation electrophoresis: 20–30 mg/L.
Cryoglobulins
Definition of Cryoglobulins
Cryoglobulins are immunoglobulin fractions that precipitate at temperatures of < 37°C and dissolve again when warmed up. They are monoclonal (type I) or mixed (types II and III; see Chap. 10, “Guillain-Barré Syndrome and Other Immune-Mediated Neuropathies”) and, like paraproteins, are associated with neuropathy.
Preanalytical requirements.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


