and Aditya G. Shivane1
(1)
Cellular and Anatomical Pathology Level 4, Derriford Hospital, Plymouth, UK
Abstract
This chapter deals with the ways in which the cellular constituents of the nervous system (neurons and glial cells) react to various insults. The severity and duration of the insult determine whether the final outcome is reversible or irreversible. Identification of these basic pathologic reactions helps the pathologist in making a diagnosis and also provides clues towards the aetiology of the pathological process.
Keywords
HypoxiaIschaemiaInclusionsGliosisPathologyThe cells which make up the nervous system and their supporting tissues can react to various insults in different ways. Many of these reactions are hard to recognise with naked eye examination and require microscopic analysis of the tissue. Sometimes, the morphology of these reactions provides clues about the aetiology of the pathological process.
2.1 Neurons
2.1.1 Neuronal Atrophy and Neuronal Loss
This is the end stage of irreversible neuronal injury. In atrophy, the cell body shrinks, cytoplasm shows diffuse basophilia and nucleus becomes dark or pyknotic. Neuronal loss is recognised by the accompanying increase in glial cells (gliosis), but sometimes may need detailed quantitative analysis. Atrophy and loss are commonly seen in aging and neurodegenerative diseases.
2.1.2 Hypoxic-Ischaemic Change
This is recognised by the presence of ‘red neurons’- shrunken neurons with bright eosinophilic cytoplasm, dark, pyknotic nuclei and loss of nucleoli (Fig. 2.1). The red neurons are not specific to hypoxia/ischaemia, but can also be seen in hypoglycaemia and excitotoxic injury. Neurons in some locations are more vulnerable to hypoxic-ischaemic injury than others e.g. pyramidal neurons of hippocampus (Sommer sector or CA1), cortical neurons (layers 3 and 5) and cerebellar Purkinje neurons. The dead neurons may sometimes be encrusted with minerals such as calcium and iron (termed ‘ferrugination’), commonly seen in infant brains with hypoxic-ischaemic injury.
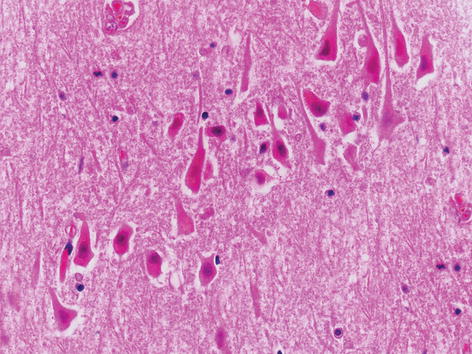
Fig. 2.1
The hippocampal pyramidal neurons showing hypoxic-ischaemic change (red neurons). H&E stain
2.1.3 Central Chromatolysis
This feature is recognised by the presence of a distended neuron with pale cytoplasm, loss of Nissl substance and eccentric location of the nucleus. This change is usually seen in lower motor neurons in the brainstem and spinal cord secondary to axonal damage. A similar change in neurons referred as ‘ballooned or swollen neurons’ can be seen in a wide variety of neurodegenerative, metabolic and developmental disorders.
2.1.4 Abnormal Inclusions
Accumulation of abnormal inclusions within a neuron (either in the cytoplasm or nucleus) (Fig. 2.2a–d) can be seen in various neurodegenerative diseases, metabolic diseases and viral infections (Table 2.1).
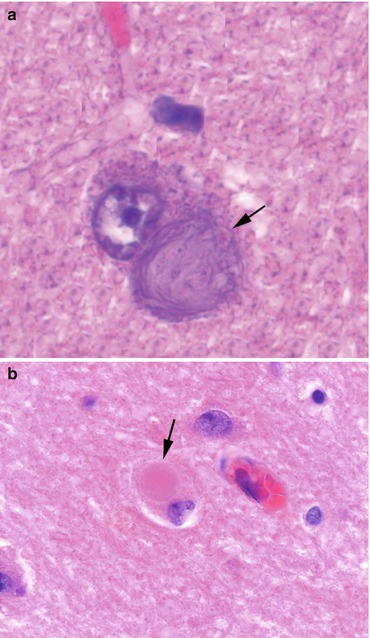
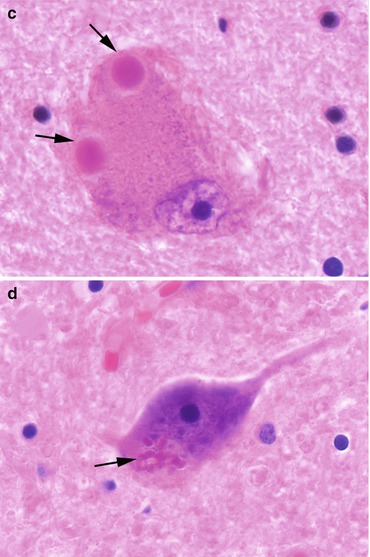
Fig. 2.2
Various abnormal neuronal inclusions (arrow). (a) Large neuron containing basophilic neurofibrillary (globose) tangle from a case of Alzheimer’s disease, (b) cortical neuron showing eosinophilic Lewy body, (c) two Lewy bodies within a substantia nigra neuron from a case of Dementia with Lewy bodies, (d) anterior horn cell neuron containing eosinophilic beaded inclusion (Bunina body) from a case of motor neuron disease
Table 2.1
Abnormal neuronal inclusions
Inclusion | Disease or association |
|---|---|
Cowdry type A & B | Cytomegalovirus, Herpes, Measles, Poliomyelitis |
Negri bodies | Rabies |
Lewy bodies | Parkinson’s disease, Dementia with Lewy bodies |
Neurofibrillary tangles | Alzheimer’s disease |
Pick bodies | Pick’s disease |
Bunina bodies | Motor neuron disease |
Lafora bodies | Myoclonic epilepsy |
Polyglucosan bodies
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





