13 Brain Metastases
Incidence
The frequency of brain metastases reflects the incidence of primary malignancy as well as the propensity for CNS dissemination. Lung, breast, melanoma, renal, and colorectal cancers account for the majority of cases of brain metastases. The overall risk of developing brain metastases in patients with solid tumors is in the region of 10%. The reported incidence for patients with lung cancer is 20%, melanoma 7%, renal carcinoma 7%, breast cancer 5%, and colorectal cancer 2%. Patients with breast cancer aged 20 to 39 years have the highest proportional risk of brain metastases.1
Presentation and Diagnosis
Patients with brain metastases may present with the classical features of a brain tumor. In the presence of multiple lesions, the presentation may be with a nonspecific global deficit and confusional state or epilepsy. Although cognitive impairment is common, detected in up to 65% of patients,2 it requires detailed neuropsychological testing. Any patient with known malignant disease presenting with any features indicating an intracranial problem requires imaging with CT, or preferably MRI, with and without contrast.
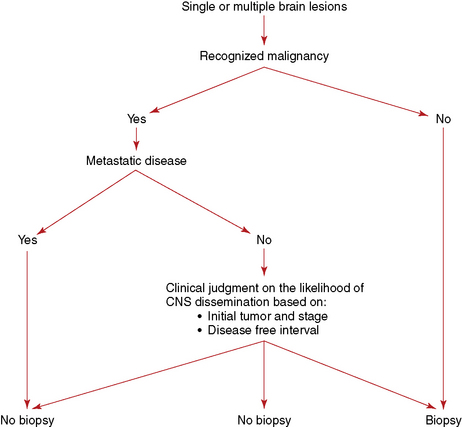
The need for a histological confirmation of metastatic disease in the brain is summarized in an algorithm (Figure 13-1). In the presence of known systemic malignancy and metastatic disease, there is no indication for biopsy of intracranial lesions unless there is a high index of suspicion for an alternative diagnosis such as an atypical infection. In patients presenting with lesions in the brain, without previous history of primary malignancy, histological confirmation of diagnosis is generally required, preferably from an extracranial site.
Prognosis
Patients with brain metastases have a limited prognosis, with few or no long-term survivors. Median survival in patients with multiple brain metastases is in the region of 3 to 4 months, and 1 year survival is in the region of 12%.3
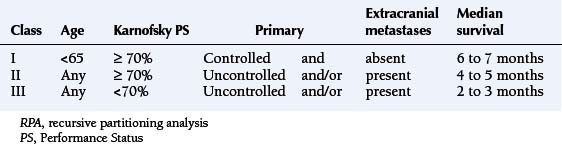
Prognostic factors for survival are performance status, age, and the presence and activity of systemic disease. Patients with all four favorable prognostic factors (Karnofsky Performance Status [KPS] >70, no extracranial metastases, controlled primary tumor, age under 65 years) have a median survival in the region of 7 months. In the presence of one adverse prognostic factor, the median survival drops to 4 months, and, if KPS score is below 70, the median survival is just over 2 months (Table 13-1).4 More recent prognostic indices also include the number of metastases, distinguishing between solitary lesions and the presence of two or three lesions or more than three.
Medical Management
The aim of treatment of brain metastases is palliation, to improve neurological deficit and quality of life and to prolong survival. Mass effect and neurological deficit assumed to be due to surrounding edema are appropriately treated with corticosteroids. Oral dexamethasone is generally employed as the drug of choice and can be administered in a single daily dose. The tendency has been to recommend a large loading dose followed by reduced daily doses, although it is not clear whether this approach leads to a faster improvement in function. The only regimen subject to a randomized trial is the administration of low-dose dexamethasone (4 mg daily) in comparison to high-dose dexamethasone (12 mg daily). The improvement in function at one week was the same regardless of dose. Patients receiving higher doses experienced more severe side effects,5 which suggests that 4 mg dexamethasone given in a single daily dose is sufficient and should only be increased in the absence of response after 2 or 3 days. In patients with clinical features of increased intracranial pressure, higher loading doses are recommended. After a clinical benefit has been achieved, the dose should be gradually titrated down to the lowest necessary to maintain improvement in symptoms. It is also important to reduce and discontinue corticosteroids after definitive treatment, to avoid cushingoid side effects.
The management of seizures in patients with brain metastases should be along the lines of management of epilepsy in patients with any brain tumor. There is no evidence for benefit of prophylactic anticonvulsants.6 If chemotherapy is part of the management (see below), it is preferable to avoid enzyme-inducing anticonvulsants that increase the metabolism of taxanes, anthracyclines, vinca alkaloids and small molecular tyrosine kinase inhibitors, leading to lower effective doses. Lamotrigine is a reasonable first choice as it does not induce liver enzymes.
Specific Treatment Modalities
SURGERY
Surgery is the appropriate treatment for accessible solitary brain metastases in noneloquent areas. The aim is complete tumor removal to obtain symptomatic relief of increased intracranial pressure or focal deficit from the tumor mass and to achieve local disease control. In patients with multiple brain metastases, surgical excision is generally not indicated, unless one large and easily accessible lesion is responsible for the majority of symptoms. Although resection of multiple brain metastases has been recommended by some authors, the apparent favorable survival seen in the reported cohorts is most likely due to patient selection rather than the efficacy of surgery.7,8
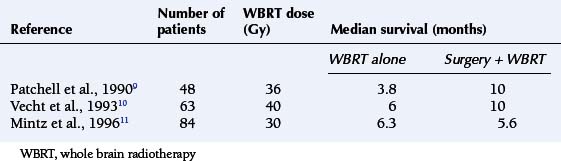
The survival benefit of surgical resection of solitary brain metastases has been tested in three small randomized trials comparing surgery and whole brain radiotherapy (WBRT) with WBRT alone. Two studies had shown prolongation in survival, but this was not confirmed in the third study (Table 13-2).9,10,11 The consensus of opinion is that surgery is the appropriate treatment for patients with solitary brain metastases, with the aim being to prolong survival and improve quality of life (QoL). However, radical excision should be reserved for patients with favorable prognostic factors, particularly those without progressive systemic disease.
RADIOTHERAPY
Whole brain irradiation has been the mainstay of treatment of patients with brain metastases. Only one randomized trial compared supportive care (corticosteroids alone) with whole brain radiotherapy (WBRT); it showed a small improvement in median survival in patients receiving WBRT.12 Subsequent randomized studies examining the role of WBRT compared different dose fractionation schedules to identify the most effective regimen. None have shown benefit for more intensive treatment employing higher doses, given either as daily fractionation or as accelerated radiotherapy using multiple treatments per day. A UK study comparing 30 Gy in 10 fractions with 12 Gy in two fractions had shown a survival benefit for longer fractionation in favorable-prognosis patients,13 and one or two fraction regimens are rarely employed. The preferred WBRT for patients with multiple brain metastases is 20 Gy in 5 fractions, or 30 Gy in 10 fractions. WBRT improves neurological function in over half of patients with a deficit, although part of the improvement may be due to corticosteroids.
It is generally accepted that patients with good performance status and reasonable prognosis may benefit from WBRT both in terms of survival and neurological function/QoL. However, the value of radiotherapy in patients with marked disability and poor performance status is questioned,14 and at present it is not clear whether WBRT is appropriate. Randomized trials currently underway examine survival and quality of life benefits of WBRT in patients with multiple brain metastases and poor prognosis.
In diseases with a high incidence of intracranial dissemination of disease, brain irradiation may be used as prophylaxis, similar to the use of craniospinal irradiation in acute lymphatic leukemia in childhood. Prophylactic cranial irradiation (PCI) improves intracranial tumor control and survival in patients with limited and advanced-stage small cell lung cancer who achieve good remission with chemotherapy15,16; however, the magnitude of gain in life expectancy is not large and neurocognitive deficits in long-term survivors are of concern. So far there is not enough evidence to support PCI in patients with other solid tumors.
RADIOTHERAPY AND RADIOSENSITIZERS
A number of radiation sensitizers have been tested in addition to radiotherapy with the aim of improving disease control in the brain as well as survival. Electron-affinic sensitizers (metronidazole, misonidazole)17,18 and sensitizers of proliferating cells (BUdr)19 have not demonstrated benefit in randomized studies. The addition of radiation sensitizers motexafin gadolinium, which is preferentially taken up by enhancing lesions,20 and efaproxiral do not improve survival or disease control.
RADIOSURGERY
Radiosurgery (stereotactic radiotherapy) is a high-precision localized radiation which can be delivered with a linear accelerator (using multiple fixed fields or multiple arcs of rotation) or with a multiheaded cobalt unit (gamma knife). Stereotactic radiotherapy delivers more localized radiation than would be achieved with conventional irradiation for lesions less than 4 cm in diameter.21
Radiosurgery has been considered as a noninvasive equivalent of surgical excision, although the apparent equivalence of tumor control and survival is based on reported data from largely retrospective phase II studies.22
Following a single radiation dose (radiosurgery) of 15 to 25 Gy, the “response rate,” measured as a reduction in the size of solitary metastases, is in the range of 80% to 90%, although complete disappearance is uncommon. In patients with MRI-proven solitary brain metastases the addition of radiosurgery to whole brain radiotherapy (WBRT) improves survival and tumor control.23 Radiosurgery does not prolong survival in patients with multiple (two or more) brain metastases.23
The prognostic factors for survival in patients with solitary brain metastases are the same as in patients with multiple brain metastases.24 The dominant adverse prognostic factor for survival is performance status.25 Patients with poor performance status and marked disability have survival similar to patients with multiple brain metastases, and radiosurgery is not appropriate as first-line palliative treatment.
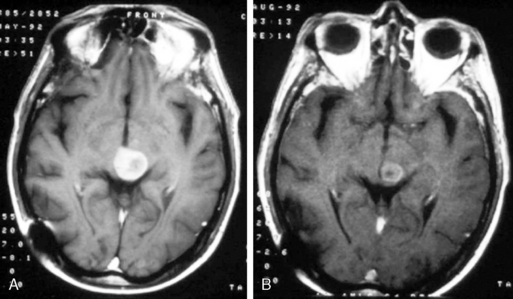
The present recommendation is to offer radiosurgery to patients with solitary brain metastases and good performance status. While it is generally reserved for patients with surgically inaccessible lesions, it can be considered as an alternative to surgery and therefore can be offered as an alternative to surgical excision even in operable lesions. It is a less invasive, less costly, and largely outpatient procedure (Figure 13-2). Radiosurgery can occasionally be offered to selected patients with two (or rarely three) metastases, good performance status, and absent or controlled systemic disease.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


