Fig. 17.1
The two-point method involves creating a point at the proposed limit of resection and one where the cavernous malformation abuts the pial surface; connecting the two points creates a line that can be extended to the cranial surface and that helps choose the appropriate craniotomy (Used with permission from Barrow Neurological Institute)
Orbitozygomatic Approach
The OZ approach is the least utilized of the five major approaches, but it is still an essential tool in the armamentarium for approaching these lesions. This approach is useful for cavernous malformation in the anterior half of the midbrain. It involves a pterional craniotomy and some variation of the OZ osteotomy (Lemole et al. 2003). The dissection involves wide arachnoid dissection of the opticocarotid cistern and a trajectory through the oculomotor-carotid window to Lillequist’s membrane. Once Lilliquist’s membrane has been traversed, the basilar artery and midbrain are exposed. Great care must be taken to avoid basilar perforators when the cavernous malformation is entered and to avoid the motor fibers of the cerebral peduncle. As in all cases, neuronavigation is useful in locating the brainstem ‘cortical’ opening point when no telling hemosiderin stain is present. The OZ approach is useful for lesions that can be accessed in the midline in the interpeduncular cistern or for lesions that can be accessed with this approach that sit lateral to the peduncle and can be removed by creating an opening in the midbrain lateral to the pyramidal tracts.
Retrosigmoid Approaches
The retrosigmoid approach is the second most commonly used approach at our institution (Abla et al. 2011). The largest proportion of cavernomas in the brainstem lies in the pons, and this approach is extremely useful in accessing these lesions. Cavernous malformations of the brainstem often expand the pons but do not reach a pial surface. The middle cerebellar peduncle, a relatively noneloquent structure, has been used to access such formidable lesions.
The middle cerebellar peduncle is often accessed behind the brainstem entry zone of the fifth cranial nerve. Staying superior is critical; an inferior entry into the middle cerebellar peduncle likely involves the seventh cranial nerve as it crosses around the sixth cranial nerve nucleus on its way to exit the brainstem in the cerebellopontine angle.
In approaching the pons in this fashion, we have abandoned more anteriorly situated craniotomies that were previously used to access the pons, including the transpetrous approaches and subtemporal approaches involving a medial petrosectomy. In our experience the retrosigmoid approach is very well tolerated and provides robust access to the pons without jeopardizing some of the more anteriorly situated motor fibers or cranial nerve nuclei. A previously reported case of an 11-year-old girl demonstrates the retrosigmoid approach (Fig. 17.2) (Abla et al. 2010a).
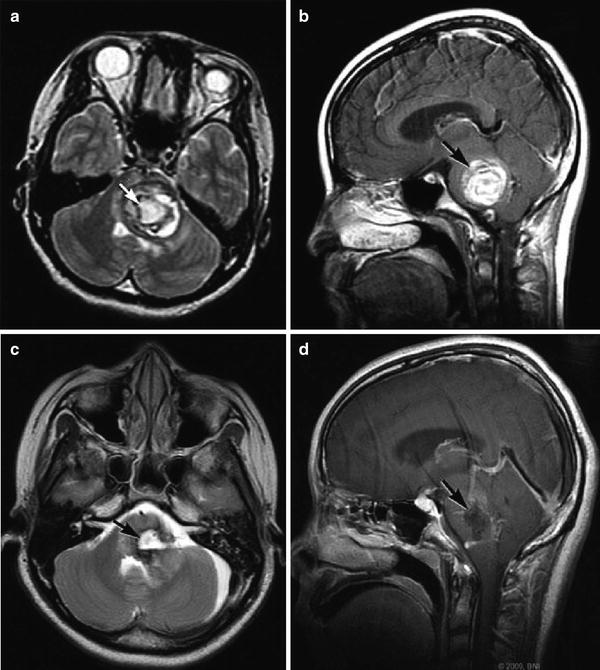
Fig. 17.2
Preoperative (a) axial T2-weighted and (b) sagittal contrast-enhanced MRI of an 11-year-old girl with a giant pontine cavernoma (arrows). Resection was performed via a left retrosigmoid craniotomy and entry through the middle cerebellar peduncle. Postoperative (c) axial T2-weighted and (d) sagittal contrast-enhanced MRIs confirm gross total resection (arrows) (Used with permission from Barrow Neurological Institute)
Lateral Supracerebellar Craniotomy
The lateral supracerebellar infratentorial craniotomy is useful for approaching cavernomas of the posterior and/or lateral midbrain. The use of the supracerebellar infratentorial approach to cavernous malformations of the brainstem in 45 patients treated at our institution has been reported elsewhere (de Oliveira et al. 2010). In that report, median, paramedian, and extreme lateral supracerebellar approaches were discussed (Fig. 17.3). Now, however, the supracerebellar approach most often used at our institution is the lateral supracerebellar approach.
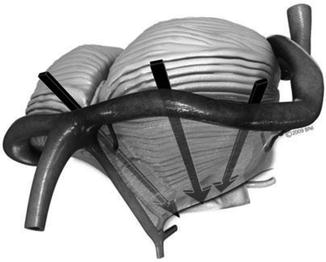
Fig. 17.3
Illustration showing three variations of the supracerebellar infratentorial approach: a median, paramedian, and extreme lateral variation (Used with permission from Barrow Neurological Institute)
This incision is placed similar to that for a retrosigmoid craniotomy, but exposure of the sigmoid sinus is not critical. The craniotomy is placed more superior to allow exposure of the transverse sinus. The craniotomy can extend superiorly above the transverse sinus. The craniotomy allows the cerebellum to be retracted inferiorly away from the transverse sinus and provides a trajectory from lateral (superficially) to more medially at the depth of the operating field usually aimed at the collicular plate.
The approach is useful for reaching lateral and posterior situated cavernomas of the midbrain. It has also been used for cavernous malformations that extend into the thalamus rostrally or into the pons inferiorly. The trochlear nerve is a useful and dependable landmark crossing around the posterior midbrain toward the ambient cistern. The park-bench position is often used (de Oliveira et al. 2010).
Far-Lateral Approach
The far-lateral approach allows access to the anterior portion of the medulla. The patient is positioned in a prone, or more preferably, a park-bench position (de Oliveira et al. 2010). A U-shaped incision was once used for this approach, but we now prefer a laterally situated vertical incision, which minimizes obstruction of the surgical corridor by the surgical flap itself.
The approach involves a suboccipital craniotomy situated lateral to a typical suboccipital opening. This approach also can involve some degree of drilling of the occipital condyle. Typically, as much as one-third of the posterior condyle can be drilled safely to increase the degree of dural retraction and a lateral-to-medial trajectory. A C1 laminectomy is also performed. The dura is opened in a curvilinear fashion and flapped laterally. Great care must be taken to avoid injury to the vertebral artery as it crosses the atlas; however, we do not routinely mobilize or skeletonize the vertebral artery in this approach to brainstem cavernomas. Dissection of the arachnoid proceeds lateral to the medulla and around the vertebral artery, twelfth cranial nerve rootlets, and the exit of the posterior inferior cerebellar artery. The brainstem is usually entered at the lateral to anterolateral aspect of the medulla.
Related posts:
 Oligodendroglial Tumors: Intra-arterial Chemotherapy
The Concept of a Preniche for Localization of Future Metastases
Resection of Brain Tumors: Intraoperative Confocal Microscopy Technology
Oligodendroglial Tumors: Intra-arterial Chemotherapy
The Concept of a Preniche for Localization of Future Metastases
Resection of Brain Tumors: Intraoperative Confocal Microscopy Technology
 Management of Hemangiopericytoma
Management of Hemangiopericytoma
 Metastatic Oligodendroglioma: Diagnosis with Fine-Needle Aspiration Cytology
Metastatic Oligodendroglioma: Diagnosis with Fine-Needle Aspiration Cytology
 Lipoma: An Overview
Lipoma: An Overview
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


