Fig. 5.1
Contrast-enhanced axial T2-FLAIR (a), axial (b), and sagittal (c) T1-weighted slices in a 31-year-old man with Brucella meningitis causing visual disturbances. Diffuse and intense enhancement in the basal cisterns after gadolinium administration, with evidence of enhancing granulomas in the interpeduncular and quadrigeminal cisterns. There is also perivascular enhancement along the course of the right middle cerebral artery. A small pontine capillary telangiectasia is evident in c
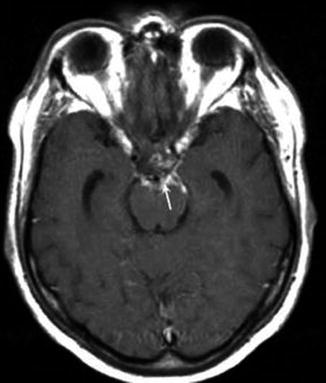
Fig. 5.2
Contrast-enhanced axial T1-weighted MRI in a 56-year-old man with Brucella meningitis causing intense headache and neck rigidity, in addition to bilateral abducens nerve palsy and amblyacousia. Note that the presence of basal enhancement of leptomeninges (arrowhead) after gadolinium administration (From Jochum et al. [19])
In the differential diagnosis of Brucella meningitis, all the infectious and noninfectious mononuclear meningitis have to be considered. Brucella meningitis should always be considered in the differential diagnosis of neurological and psychiatric cases that are encountered in endemic areas for brucellosis [15, 16, 20].
5.8 Prognosis
Brucella meningitis differs from other forms of chronic meningitis because it has a better prognosis; in fact mortality is generally lower, with disease being rarely fatal (<0.5) with proper management, and the cause of death is not always clearly related to brucellosis. On the contrary, patients who suffered from diffuse CNS involvement (severe encephalic or spinal cord disease) had a worse prognosis, with mortality not negligible and frequent sequelae. Meningovascular complications, in particular mycotic aneurysms, ischemic stroke, venous thrombosis, and subarachnoid hemorrhage, are relatively common. The incidence of minor sequelae is high and will increase in case of a delay in treatment; however, only a few patients suffered important limitations in their normal activity [4, 20].
5.9 Treatment
There is still no agreement for choice of antibiotic, dose, and time of the treatment of neurological involvement by Brucella spp. [4]. Monotherapy can cause relapses, from 40 to 80 %; therefore, combined dual or triple combination therapy with doxycycline, rifampicin, trimethoprim-sulfamethoxazole (TMP/SMZ), streptomycin, or ceftriaxone for >2 months is recommended. Ciprofloxacin combined with other antibiotics is as effective as the standard regimen of doxycycline and rifampicin [5, 7, 10].
Cranial nerve palsies compared during acute infection usually resolve completely with therapy, whereas those with chronic CNS infection often have permanent neurological deficit [3, 4, 33]. Some authors suggest that antibiotic treatment has to be continued until improvement of clinical symptoms, glucose normalization in CSF, reduction of leukocytes less than 100 cells/mm3, and the decrease of antibody titers [3].
Conclusion
Brucella bacteria can cause meningitis directly or through invasion of immunologic cell system.
Pathological changes of the meninges are frequent.
The clinical presentation of meningitis is various; however, the most common neurological symptoms are headache, nausea, and/or vomiting, and the chief signs are nuchal rigidity, Kernig’s sign, Brudzinski’s sign, confusion, and altered consciousness.
In the literature, diagnostic criteria are problematic, and the diagnosis is based on clinical and laboratory exams.
The prognosis quoad vitam is better than the other forms of chronic meningitis; mortality is generally low, but the prognosis quoad valetudinem is low; the incidence of minor sequelae is high and will increase in case of a delay in treatment.
Dual or triple combination therapy with doxycycline, rifampicin, TMP/SMZ, streptomycin, or ceftriaxone for >2 months is recommended.
References
1.
Al-Sous MW, Bohlega S, Al-Kawi MZ, Alwatban J, McLean DR (2004) Neurobrucellosis: clinical and neuroimaging correlation. AJNR Am J Neuroradiol 25:395–401PubMed
2.
3.
4.
5.
6.
Corbel MJ (1997) Brucellosis: an overview. Emerg Infect Dis 3:213–221PubMedCentralPubMedCrossRef
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


