25 | C1 Ring Fractures |
 | Case Presentation |
History and Physical Examination
A 27-year-old male with a history of psychiatric disorders fell down a flight of stairs and presented to the emergency department with complaints of neck and shoulder pain. There was no loss of consciousness and his neurological examination revealed no deficit. A separation of the acromioclavicular joint was diagnosed on the right.
Radiological Findings
Computed tomographic (CT) reconstruction of the cervical spine revealed a displaced burst fracture of C1 (Fig. 25–1). The relationship between the anterior C1 ring and the odontoid remained anatomical, indicating that the transverse ligament remained intact.
Diagnosis
C1 ring burst fracture (Jefferson fracture) with intact transverse ligament
 | Background |
Fractures of the atlas represent ~10% of all cervical fractures, half of which are associated with other spinal injuries, most commonly, the axis. Because of the large spinal canal area at this level, neurological injuries are relatively infrequent.
Fractures of the atlas can typically be identified from plain radiography, although in most modern trauma settings, spiral CT has replaced plain x-rays, with increased sensitivity and specificity. A lateral view may identify injuries to the posterior arch, whereas an open-mouth view evaluates the relative position of the articular masses.
Fractures of the atlas may be considered either stable or unstable, depending on the location of the fracture, the degree of comminution, and how displaced the fracture fragments are. Fractures isolated to the posterior arch and those minimally displaced fractures of the anterior ring can usually be treated quite successfully with brace or collar immobilization. Fractures of the lateral masses may be (1) impaction fractures wherein the ring integrity is preserved, or (2) comminuted with separation of the masses and loss of stability.
Bursting fractures may be associated with failure of the transverse ligament and permit lateral mass subluxation and loss of ring integrity. “Blowout” fractures of the anterior arch or true Jefferson burst fractures are felt to be unstable and should be considered for either halo or surgical stabilization. Halo stabilization is certainly adequate as long as the transverse atlantal ligament is intact. Levine and Edwards1 have suggested that an open-mouth view of the Jefferson fracture that shows less than 7 mm of lateral mass spreading can be considered stable and treated with immediate halo application and mobilization. Lee et al have even reported quite satisfactory treatment of stable Jefferson fractures with 10 to 12 weeks of rigid cervical collar alone.2
If the transverse ligament has been disrupted and is not competent (e.g., more than 7 mm of lateral mass spreading on radiography) once the patient becomes upright and mobilized in the halo, the fracture fragments and lateral masses will splay out laterally. In this situation surgical stabilization is most commonly considered. An alternative is prolonged recumbent traction of up to 6 weeks before the patient becomes mobilized1; however, the risks of prolonged bed rest must be carefully understood.
Dickman et al3 further differentiated transverse ligament disruptions into primarily ligamentous (type 1) injuries and those with principally bony avulsion of the ligamentous connection (type 2). Their recommendations have been that those with primarily ligamentous failure be treated with surgical arthrodesis, whereas bony avulsion fractures could be treated with rigid external immobilization. A failure rate of over 20% has been noted, however.
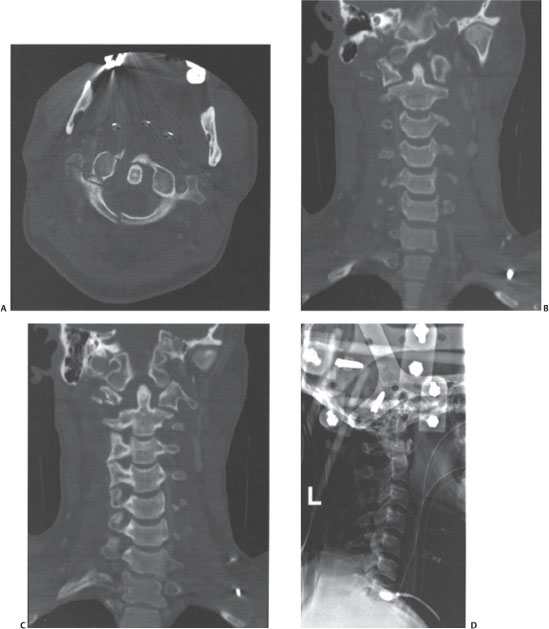
Figure 25–1 (A) Axial computed tomographic image of a Jefferson burst fracture of the ring of C1 with extension into the vascular foramen on the right. (B) Coronal images demonstrating minimal splaying of the lateral masses. (D) Lateral radiograph of the cervical spine after halo application.



