Chapter 8 The polysomnogram (PSG) provides a good opportunity to evaluate cardiac rhythms. Although medically threatening abnormalities are seen less frequently today than in the past, sleep specialists and technicians must be able to recognize the basic abnormalities. This chapter highlights some of the cardiac arrhythmias seen during overnight PSG recording (Figs. 8.1 to 8.13). FIGURE 8.1 Severe disease-related bradyarrhythmia in rapid eye movement (REM) sleep. FIGURE 8.2 Ventricular ectopy in rapid eye movement (REM) sleep. FIGURE 8.3 Second-degree heart block, Wenckebach. FIGURE 8.4 Supraventricular tachycardia.
Cardiac Arrhythmias

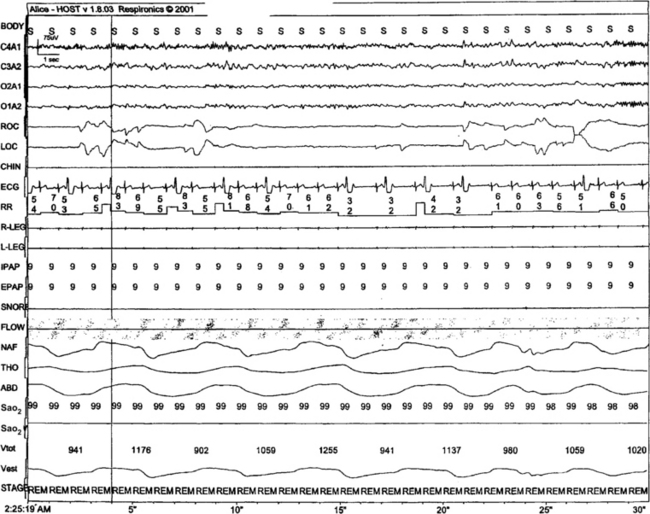
A 56-year-old man with severe daytime sleepiness. The left side of the snapshot shows a heart rate less than 50 beats/min, the termination of an apnea, and severe hypoxia (saturation in the mid-70s). Just before the arousal there is a 4-second period with no electrocardiographic (ECG) rhythm (possible sinus arrest or sinoatrial exit block), followed by a ventricular escape, and postarousal tachycardia, with a near doubling of heart rate. The ECG R-wave amplitude also shows fluctuations that track respiratory effort: This ECG-derived respiration signal is secondary to changes in the cardiac axis generated by positional variation of the heart in the thoracic cavity associated with respiration.
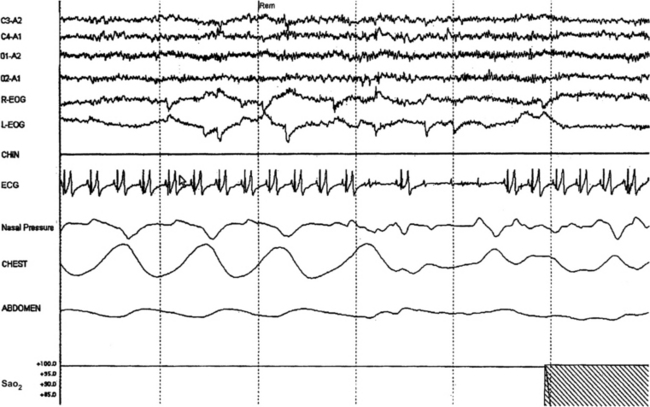
Bigeminy and trigeminy are noted in this 26-year-old woman who presented with nonhypoxic obstructive sleep-disordered breathing. This finding was not seen in non-REM (NREM) sleep. There was excessive use of caffeine (four to five large cups of strong coffee across the day). The patient has no palpitations during the day or night.
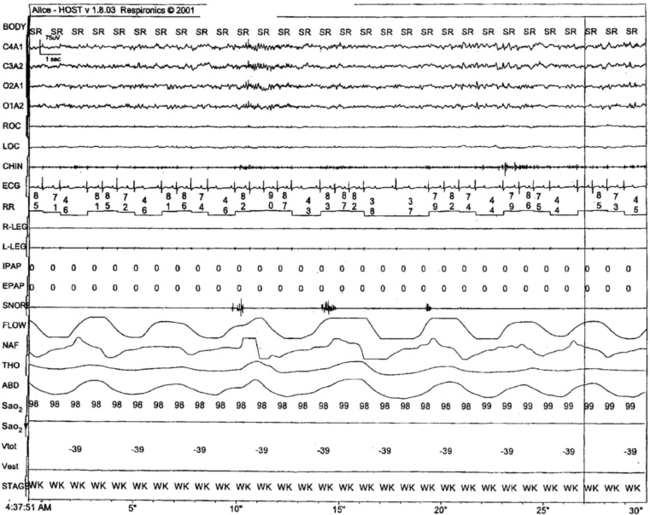
Progressive increase in PR interval preceding dropped beats in a 48-year-old patient with delayed sleep phase disorder, seen unchanged during wake and sleep. This is an innocent arrhythmia and requires no treatment.
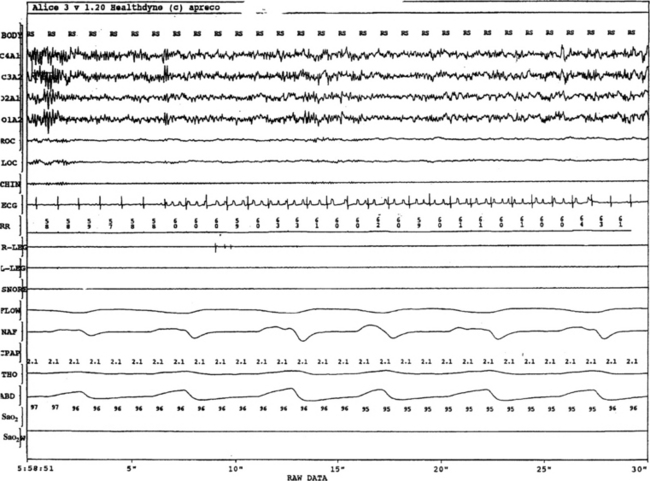
Atrial tachycardia with varying block or a run of atrial flutter with varying block. The abrupt change in P-wave morphologic characteristics is not associated with any change in QRS morphologic characteristics. The ability of a single ECG channel in precisely determining the origin of rhythms can be limited. This patient was not on any medication such as digitalis.
< div class='tao-gold-member'>
Related posts:
 1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
 4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
 Motor Disorders During Sleep
Motor Disorders During Sleep
 Oral Appliances and Surgical Techniques for Obstructive Sleep Apnea Syndrome Therapy
Oral Appliances and Surgical Techniques for Obstructive Sleep Apnea Syndrome Therapy
 Specialized Techniques
Specialized Techniques



