14
Central Sleep Apnea
JOANNE HEBDING
Note: This chapter corresponds to Chapter 17 in Fundamentals of Sleep Technology, 2nd edition.
1. A 93-year-old Caucasian man has increasing shortness of breath when walking to and from his house. He reports a history of loud snoring and excessive sleepiness. He habitually goes to bed at 11:30 pm and wakes up at 8:00 am, for a nightly sleep duration of 9.5 hours. Although he sleeps well and wakes up feeling refreshed, he falls asleep when sitting down or watching television. He described needing to go to the bathroom several times during the night.
He has a history of hypertension, coronary artery disease (myocardial infarction), atrial fibrillation, and sick sinus syndrome. He was undergone pacemaker placement and coronary artery bypass graft surgery. A lifelong nonsmoker, he has no known lung disease.
Physical examination reveals a BMI of 28.8 kg/m2 and bibasilar crackles. Overnight oximetry shows repetitive sawtooth-pattern oxygen desaturation with a lowest oxygen saturation (SaO2 min) of 76%.
A split-night polysomnogram demonstrates the following respiratory events (Fig. 14.1).
Which of the following will be most effective in eliminating these respiratory events?
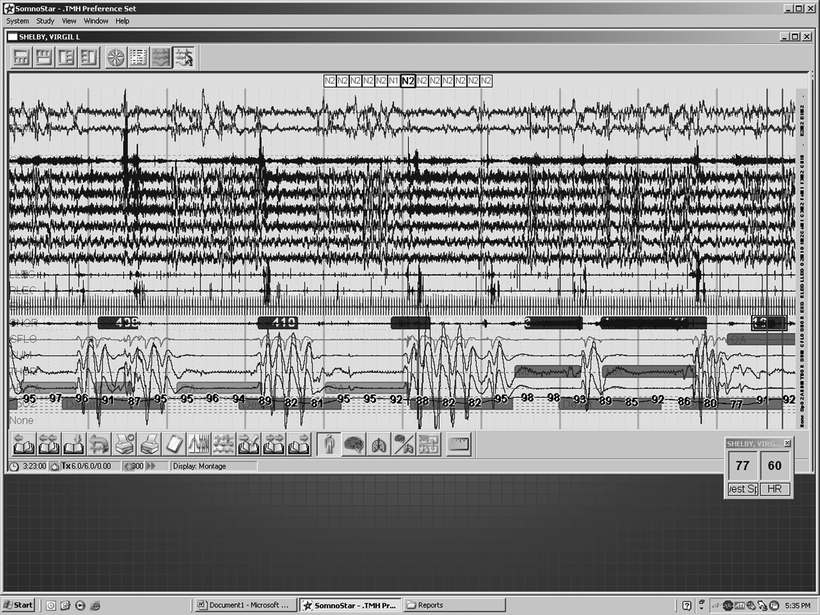
Figure 14.1 Five-minute window.
A. Continuous positive airway pressure (CPAP)
B. Bilevel positive airway pressure (BPAP)
C. BPAP with a backup rate or adaptive servo ventilation (ASV)
2. All of the following respiratory patterns are classified as central sleep apnea, except:
A. Cheyne-Stokes respiration
B. High-altitude periodic breathing
C. Obesity hypoventilation syndrome
D. Complex sleep apnea
3. A patient undergoing a split night sleep study has obstructive apneas and hypopneas, and an apnea hypopnea index (AHI) greater than 40 events per hour. Central events are rare at baseline but increased during continuous positive airway pressure (CPAP) titration in stages N2 and N3 sleep. What type of central apnea is most likely present in this patient?
A. Hypercapnic central sleep apnea
B. Cheyne-Stokes respiration
C. Complex sleep apnea
D. Sleep-onset periodic breathing
4. Hypercapnia is an essential feature of all hypoventilation syndromes. True or false?
5. Which of the following is a cause of hypercapnic central sleep apnea?
A. Heart failure
B. High altitude
C. Neuromuscular disorder
D. Onset of sleep
6. Cheyne-Stokes respiration (CSR) is characterized by which type of respiratory pattern?
A. Irregularly regular
B. Relaxed–narrowing
C. Waxing–waning
D. Repetitive–staccato
MATCH THE TERM WITH ITS DEFINITION
| 7. | Central sleep apnea | A. | Abnormally high CO2 levels |
| 8. | Complex sleep apnea | B. | Can give rise to obstructive and central sleep apnea as well as Cheyne-Stokes respiration |
| 9. | Hypercapnia | C. | Automatic airflow-targeted ventilation |
| 10. | Hypoventilation | D. | Abnormal respiratory patterns, including hypoventilation, central apnea, and Biot breathing |
| 11. | Cheyne-Stokes respiration | E. | Application of continuous positive airway pressure (CPAP) for obstructive sleep apnea elicits central apneas |
| 12. | Congestive heart failure | E. | Slow and/or shallow breathing that results in increased CO2 levels |
| 13. | Central nervous system dysfunction | G. | Cessation of breathing with absence of airflow and effort |
| 14. | Positive airway pressure therapy | H. | Rhythmic waxing and waning of breathing with regularly recurring central apneic periods |
| 15. | Adaptive servo ventilation | I. | Pressure delivered in increments of cmH2O |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


