Chapter 112 Cervicothoracic Junction Tumors
Regional Challenges
Incidence and Statistics
The upper thoracic vertebrae account for 15% of patients with tumors of the spine. The T1-4 region accounts for 10% of all spinal metastases.1 Subaxial cervical spine tumors also are uncommon and constitute less than 10% of spinal metastases.2 Due to the smaller canal size, tenuous blood supply at the cervicothoracic junction, along with unique biomechanical stresses that can lead to instability, the chance of neurologic involvement can be as high as 80%.3
The cervicothoracic junction is a transition zone between the more mobile cervical spine, with its lordotic alignment, and the much stiffer, kyphotic thoracic spine, stabilized ventrally by the rib cage. A variety of pathologic entities that can result in kyphotic deformity can be seen at the cervicothoracic junction, including tumor, infection, spondylosis, traumatic injury, and iatrogenic destabilization. Following surgery, the kyphotic deformity may worsen further as a result of failing to account for the unique biomechanics of the cervicothoracic junction.4 Cervicothoracic pathology can include either primary or metastatic oncologic disease. Several studies have looked specifically at tumors in this anatomic region.5–7 One series of 19 patients with cervicothoracic tumors had 6 patients with primary pathology, including angiosarcoma,1 chordoma,1 lymphoma,2 plasmacytoma,1 and schwannoma.1 The other 13 patients (68%) had metastatic disease, with metastases to the lung5 and prostate2 being the most common. Other tumors seen were breast cancers, melanoma, and renal, ovarian, and colon cancers. Another series with 32 patients described 19 who had lung cancer and vertebral body invasion (Pancoast tumors), 11 with metastasis, 1 with chondrosarcoma, and 1 with myeloma.6 An and Vaccaro7 reported a group of 15 patients with cervicothoracic pathology, including 8 metastatic lesions (2 breast, 2 lung, 2 prostate, 1 thyroid, and 1 adenocarcinoma of unknown origin) and the remainder primary benign (aneurysmal bone cyst, giant cell tumor) and malignant tumors (myeloma, lymphoma, neurofibrosarcoma, and hemangioendothelioma).
Nonsurgical and Surgical Treatment
Spinal metastases, especially at the cervicothoracic junction, present unique treatment considerations. The goal of treatment is to improve or maintain neurologic function, achieve spinal stability, and attain local tumor control. The traditional methods of dealing with this pathology include radiation therapy, chemotherapy, and hormonal treatment, as well as surgery. Bilsky et al.8 expanded on the NOMS pneumonic (neurologic, oncologic considerations, mechanical instability, and systemic disease and comorbidities), developing an algorithmic approach to decision making.
Radiation, Chemotherapy, and Stereotactic Radiosurgery Preoperatively and Postoperatively
The ultimate goal of treatment in patients with cervicothoracic tumors is preservation or recovery of neurologic and functional status and treatment of pain. Although radiation is less invasive, has fewer complications, and traditionally has been found to be at least equivalent to surgery for the treatment of metastases, patients with epidural spinal cord compression have been shown to respond well to surgical intervention.9 Initially, basic decompressive procedures, such as laminectomy without instrumentation, were used to resect epidural disease, although these procedures did create iatrogenic instability. Patients receiving radiation therapy as a primary treatment had 79% maintenance of ambulatory status and a 42% rate of neurologic recovery. By comparison, patients undergoing surgical intervention as mentioned above had worse odds of improving their preoperative neurologic status, with 33% chance of recovery and up to 50% of the patients worse off neurologically.10,11
In 1978, Gilbert and colleagues compared radiation therapy directly with laminectomy alone. They showed that patients with radiosensitive tumors, including breast cancers, myeloma, and lymphoma, had significantly better functional outcomes when compared with less radiosensitive tumors, including lung, colon, and renal cell carcinoma, regardless of the tumor treatment. Gilbert et al. helped steer primary treatment in certain metastatic diseases to radiation therapy.12
In general, surgical resection of epidural metastases, if tolerated well from a medical standpoint, should be followed by radiation therapy, or possibly systemic chemotherapy or hormonal therapy. This combined approach can be used to secure local tumor control.9 Newer techniques, including image-guided intensity-modulated radiation therapy (IGIMRT) and the cyberknife, improve the chances for tumor control in the cases of radiation therapy–resistant tumors, especially postoperatively, as opposed to conventional external-beam radiation therapy (EBRT).13,14 At Memorial Sloan-Kettering Cancer Center, the typical tumor board protocol currently dictates that a patient with a radiosensitive tumor, regardless of the degree of spinal cord compression or myelopathy, be irradiated with standard EBRT or with single-fraction IGIMRT or chemotherapy for noncompressive masses. Patients with radioresistant tumors and a low degree of compression can undergo EBRT or IGIMRT 24-Gy single fractions, whereas the patients with higher-grade spinal compression are offered surgical decompression and fixation followed by IGIMRT.8 Despite diligent treatment, the chance of recurrence in some of the surgical series remains high, approaching 96% at 4 years.15
Superior sulcus non–small-cell lung carcinomas, which are extremely difficult to treat because of their aggressiveness and invasion of adjacent spine, brachial plexus, and subclavian vessels, have been treated traditionally with radiation and surgery, yielding a 30% 5-year survival rate. More recent data suggest that induction chemoradiation (two cycles of cisplatin and etoposide with radiation) and surgical resection (thoracotomy) followed by two more cycles of chemotherapy can yield higher survival rates, of 44% at 5 years.16
Surgical Treatment
Surgical treatment of tumors of the cervicothoracic junction often is challenging due to the presence of major vascular and soft tissue structures requiring exquisite preoperative planning and approach. The cervicothoracic junction is unique biomechanically. This uniqueness must be accounted for when considering surgery in this region. Preoperative imaging helps define the neurovascular involvement of the tumor, guiding the direction of the surgical treatment. In the cervical spine, for example, MRI can help identify epidural spinal cord compression and vertebral artery involvement. Preoperative angiography and balloon occlusion tests may be necessary if tumor dissection or occlusion of a single vertebral artery is likely or necessary.17 For ventral surgical approaches to the subaxial cervical spine and cervicothoracic junction, the recurrent and superior laryngeal nerve functions must be evaluated. Preoperative laryngoscopy can be used to assess bilateral vocal cord dysfunction; if present, the approach should be from the ipsilateral side. Superficial laryngeal nerve function must be evaluated by swallowing studies.
Although radiation therapy remains the treatment of choice for many patients with metastatic disease, 17 primary malignant tumors often are treated surgically for oncologic considerations, because they can be resistant to chemotherapy and radiation therapy. En bloc resection, which offers a higher probability of cure and local disease control, is preferred, but it typically is more technically demanding than an intralesional resection, especially if it extends beyond the vertebral body or dorsal elements. It may occasionally entail sacrificing the adjoining vertebral artery or an exiting nerve root.
Ideally, most hypervascular spinal tumors should undergo arterial embolization prior to surgical resection to minimize the risk of intraoperative and postoperative bleeding and enhance the surgeon’s ability to safely decompress the spinal cord and maximize tumor removal.18–20 The need for preoperative embolization is based on tumor histology, as seen in renal cell carcinoma, sarcomas (e.g., angiosarcoma and leiomyosarcoma), follicular and papillary thyroid carcinoma, hepatocellular carcinoma, germ cell tumors, and neuroendocrine tumors such as paragangliomas. The arterial blood supply must be conducive to such an attempt, because the feeder vessels must be large and accessible for microcatheterization. Some other hypervascular tumors, such as melanoma and multiple myeloma, are fed by a finer capillary network, which may not be as accessible.18 On MRI, tumor hypervascularity may be identified as bright contrast enhancement and flow voids representing blood vessels. Hyperintensity also may be present on both T1- and T2-weighted images due to extracellular methemoglobin or hypointensity from the breakdown products of methemoglobin. Prabhu et al.18 have recommended preoperative angiography for the following circumstances: if the tumors are of known hypervascularity, regardless of MRI findings; if the MRI suggests hypervascularity regardless of histology; or if the primary tumor origin is unknown. Cervical tumors need special consideration, because there is an increased risk of cerebral or brainstem infarction with preoperative embolization.21 Two percent of patients experience neurologic complications, and 4% to 10% can experience local or systemic complications following embolization.18 Therefore, only in special circumstances is embolization used for cervical malignancies.
Historical Surgical Approaches
Ventral surgical approaches to the thoracic spine initially were developed to treat Pott disease, and similar principles are used today to treat primary and metastatic tumors of the spine, with the cervicothoracic junction being the most challenging. Menard22 was the first to describe an approach to this pathology; he resected a portion of the rib and transverse process to gain access to a relatively small portion of the vertebral body. Capener23 took this approach a step further by removing a longer segment of the rib, resulting in a more generous exposure and allowing ventrolateral decompression of the spinal cord.
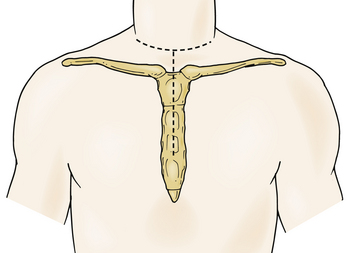
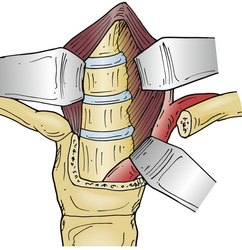
In 1957, Nanson24 described an oblique approach at the cervicothoracic junction that used a supraclavicular incision to gain access to the upper thoracic sympathetic ganglia. The exposure of the vertebral bodies, however, was very limited. Cauchoix and Binet25 described a more aggressive approach to the cervicothoracic junction that involved performing a median sternotomy. This approach was essentially abandoned due to the 40% mortality rate in patients with Pott disease26 and a 33% mortality rate in patients with cervicothoracic pathology.3 In 1984, Sundarsan et al.27 described a ventral approach, which involves a T-shaped incision with the transverse portion just proximal to the clavicles and a vertical component in the midline over the sternum (Fig. 112-1). Flaps are raised superiorly and inferiorly, and the external jugular vein and medial supraclavicular nerve are divided. The medial one third of the clavicle is excised, as well as a rectangular block of bone from the sternum (Fig. 112-2). Under the manubrium sterni the subclavian vein is dissected free, and the thymus may be removed for further exposure. The laryngeal nerve must be identified as the dissection continues deep between the carotid sheath laterally and the esophagus medially. The resected clavicle can be used as structural bone graft at the corpectomy site without further instrumentation.27
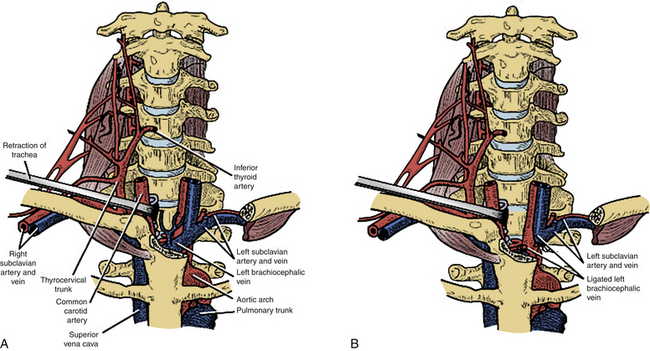
This approach was slightly modified by Birch et al.,28 who described an osseomuscular flap containing the medial one third of the clavicle and manubrium in one piece attached to the sternocleidomastoid muscle and later reattached with wires and plate-screw fixation. There were four clavicle nonunions and one transient recurrent laryngeal nerve palsy in the 17 patients in this study. By leaving the sternocleidomastoid muscle attached, the risk of pulmonary compromise was lowered in patients with respiratory problems. Kurz and Herkowitz29 modified this approach by only removing the medial clavicle without resecting the manubrium. Midline-crossing vascular structures limit exposure caudally to approximately T3 (Fig. 112-3). The lateral extracavitary approach to traumatic lesions of the thoracic and lumbar spine has been described for approaches as high as T3 but has limited utility with cervicothoracic junction tumors.30
Ventral “Trapdoor” Approach
The “trapdoor” exposure to the cervicothoracic junction has the advantage of leaving the sternoclavicular junction as well as the clavicle itself intact. Originally described by Nazzaro et al.,31 it is a combination of the ventrolateral cervical approach, median sternotomy, and ventrolateral thoracotomy. This approach is ideal for patients with ventral pathology at the cervicothoracic junction down to the T3-4 level who need decompression and subsequent reconstruction. Patients undergoing the procedure must have their neurologic status closely monitored with motor and somatosensory-evoked potentials and intravascular volume status with the help of a central line or Swan-Ganz catheter. Lines should not be placed in the right internal jugular or subclavian vein, which will be in the field,32 assuming a right-sided approach is utilized.
The incision is made along the ventral border of the sternocleidomastoid muscle on the right side, to the sternal notch and down to the level of the fourth intercostal space, lying over the midline of the sternum and then curving laterally over the fourth rib. Proximally, the dissection is taken deep in the usual Smith-Robinson technique33 by incising the platysma muscle and staying in the avascular plane between the carotid sheath laterally and the tracheoesophageal viscera medially. It may be necessary to transect or ligate the omohyoid muscle and the middle thyroid vessels in order to obtain a wider exposure. Once the prevertebral fascia is reached overlying the ventral cervical spine, the longus colli muscles are visualized. Distally, a plane is identified between the manubrium and the underlying vascular structures. Once the right lung is deflated, the sternum is transected longitudinally to the level of the fourth rib, and the incision is connected to the laterally made thoracotomy dissection. A chest spreader is used to obtain deep access. The mammary artery is identified; this artery typically requires ligation.
Lateral Parascapular Extrapleural Approach
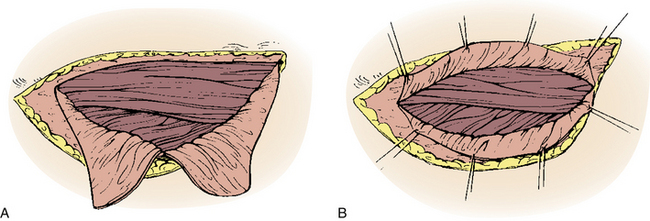
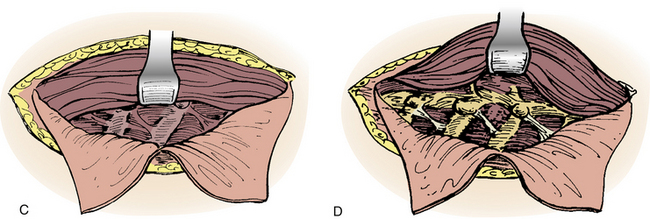
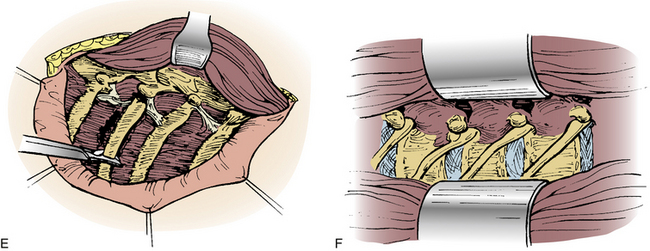
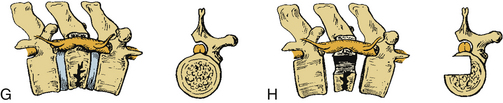
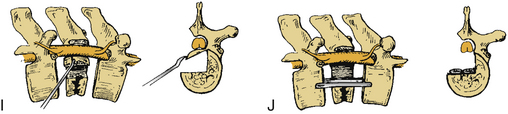
A straight ventral approach occasionally should be supplemented by a dorsal approach to allow for supplemental instrumentation or decompression. In 1991, Fessler et al.34 described a lateral parascapular approach to the cervicothoracic junction that allowed access to the anterior column of the spine and simultaneous placement of dorsal instrumentation. The patient is intubated with a double-lumen endotracheal tube and placed prone on chest rolls. (We often do not use a double-lumen tube.) The incision is begun midline over the spinous processes of the subaxial cervical spine and directed distally in a curved fashion to the ipsilateral scapula. The trapezius and rhomboid muscles are identified under the deep fascia and elevated subperiosteally toward the medial border of the scapula as a musculocutaneous flap, with the interspinous ligaments and a cuff of muscles left intact for approximation later. The intact paraspinal muscles (the spinalis thoracis and longissimus thoracis) are elevated and retracted dorsally and medially. The ileocostalis group of the erector spinae musculature can be elevated and retracted either medially or laterally. These steps provide the surgeon with an excellent exposure of the upper dorsal rib cage and dorsal vertebral elements (Fig. 112-4).
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


