Fig. 1
Development of PtiO2 in the left frontal lobe during endovascular intervention. Times for PTA in the left and right internal carotid artery and period of nimodipin administration are indicated
Case 2
A 54-year-old man developed a mild right-sided hemiparesis and confusion 6 days after SAH, and CT angiography revealed vasospasm bilaterally. Figure 2 shows the development of PtiO2 in the left frontal lobe during anesthesia, verapamil infusion, and bilateral PTA. A decrease in MAP after anesthesia made the use of vasopressor agents (ephedrine and phenylephrine) necessary. After initiation of continuous phenylephrine infusion, PtiO2 values decreased to near zero. No immediate effect of intraarterial verapamil was observed; the PtiO2 rose to normal levels and even to values suggesting hyperperfusion (>80 mmHg) only after PTA. Angiography after the intervention showed resolution of the vasospasm.
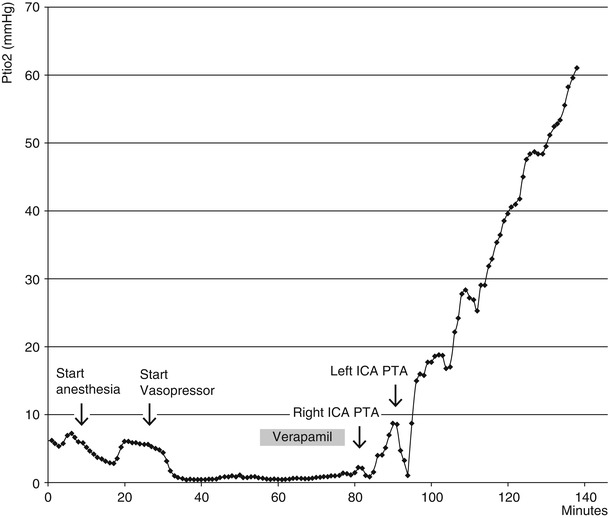
Fig. 2
PtiO2 values in the left frontal lobe during endovascular intervention. Times for anesthesia, vasopressor administration, intraarterial verapamil administration, and PTA are indicated
The increased PtiO2 values obtained during intervention were not lasting. Within 24 h after intervention, PtiO2 decreased to the level observed before the intervention and even below. Clinically, a dramatic worsening was observed after the intervention in this case. The mild paresis worsened to paralysis and the Glasgow Coma Scale (GCS) dropped from 14 to 6. CT scan revealed infarction in the left frontal lobe.
Case 3
Figure 3 shows PtiO2 values during administration of vasopressor agents and intraarterial administration of nimopidin (2 mg in the ICA, bilaterally). A significant drop in PtiO2 is observed after administration of vasopressor agents. After nimodipine administration, the PtiO2 level rose to the preintervention level, but not above. No clinical improvement was seen after the intervention.
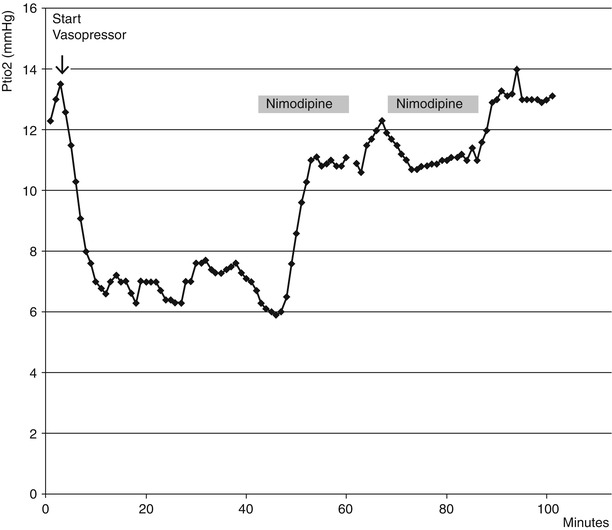
Fig. 3
PtiO2 values in the left frontal lobe during endovascular intervention. Times for vasopressor administration and intraarterial nimodipin administration are indicated
Discussion
The above cases show that decreases in PtiO2 values can be dramatically improved by mechanic/pharmacological dilation of the main cerebral arteries. However, no clinical improvement was seen in any of the cases. Several reasons can account for this. In Figs. 1 and 3, very low levels of PtiO2 are seen during the intervention. In Fig. 1, the PtiO2 level dropped to values below 2 mmHg for several minutes as the feeding artery was manipulated during PTA. No vasopressors were used in this case. In Fig. 3, a dramatic drop in PtiO2 to near 0 mmHg was seen after initiation of vasopressor agents. The curves suggest that both manipulation of the arteries and the use of vasopressors in patients with cerebral vasospasm can cause ischemia, potentially leading to poorer outcome than without any intervention.
Related posts:
 Role of Erythropoietin in Aneurysmal Subarachnoid Haemorrhage: From Bench to Bedside
Modulation of Spreading Depolarizations
Factors of Temporary Arterial Occlusion During Anterior Communicating Artery Aneurysm Repair
Impairment in Aneurysmal Subarachnoid Hemorrhage Patients with Delayed Cerebral Infarction: Prevalence and Pattern
Role of Erythropoietin in Aneurysmal Subarachnoid Haemorrhage: From Bench to Bedside
Modulation of Spreading Depolarizations
Factors of Temporary Arterial Occlusion During Anterior Communicating Artery Aneurysm Repair
Impairment in Aneurysmal Subarachnoid Hemorrhage Patients with Delayed Cerebral Infarction: Prevalence and Pattern
 Intracranial Arterial Pressure Monitoring During Endovascular Cerebral Aneurysms Embolization for Cerebral Perfusion Evaluation
Intracranial Arterial Pressure Monitoring During Endovascular Cerebral Aneurysms Embolization for Cerebral Perfusion Evaluation
 Secondary Injury After Subarachnoid Hemorrhage in Light of Multimodal Advanced Neuroimaging, Intracranial and Transcranial Neuromonitoring: Beyond Vasospasm
Secondary Injury After Subarachnoid Hemorrhage in Light of Multimodal Advanced Neuroimaging, Intracranial and Transcranial Neuromonitoring: Beyond Vasospasm
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


