Classifications of Bone Tumors of the Spine
Stefano Boriani
Stefania Paderni
Alessandro Gasbarrini
Michele Cappuccio
Luca Boriani
Stefano Bandiera
ABSTRACT
Background
Any classification discards details and therefore modifies reality, but classifications are needed in medicine to create categories associated with similar behavior and evolution. This is mandatory for the decision-making process.
Methods
We describe currently accepted classifications of primary and secondary tumors of the spine.
Results
The basic classification of spine tumors is histologic, but for the decision-making process, a scale of aggressiveness is needed.
Conclusions
The Enneking staging system (10) proved to be a reliable method to understand the biologic behavior of primary bone tumors. Many scoring systems have been proposed for grading metastases, but no consensus has been reached. A flow-chart is proposed to articulate the patient’s priorities with treatment options.
INTRODUCTION
Primary bone tumors of the spine are rare, often unsuspected, and misdiagnosis or late diagnosis is an unfortunate reality in many cases. Conversely, bone metastases in the spine are much more frequent: a 20% to 70% incidence of spine metastasis is reported in the evolution of the more common solid tumors. The magnitude of clinical problems due to spine metastases is revealed by the incidence of paraplegia in the population (8.5 per 100,000) versus traumatic spinal cord injuries (three to five per 100,000) (24). The main concern in the treatment of spine metastases is preserving mechanical and neurologic function (and deleting pain), whereas an oncologically appropriate treatment (based on early diagnosis and staging) can substantially improve the prognosis in primary bone tumors.
Classifications are needed in medicine to create categories associated with similar behavior and evolution, to set up proper decision-making processes. Any classification discards details and therefore modifies reality, but this generalization is mandatory to decide the treatment and evaluate the results.
PRIMARY TUMORS
According to the classification proposed by Schajowicz (20,21) and accepted by the World Health Organization, bone tumors are divided according to their histogenesis (Fig. 2.1).
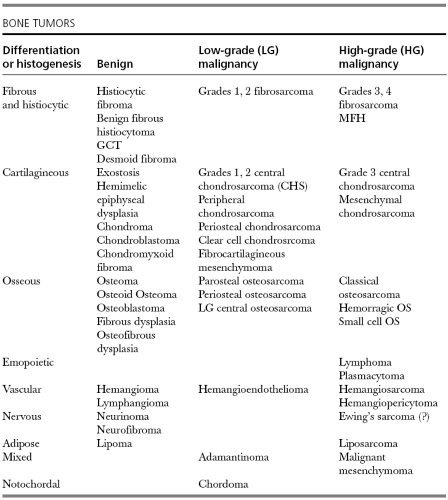 FIGURE 2.1 Histogenetic classification (with some minor changes) of the World Health Organization by Schajowicz et al. (1972) for tumors of the skeleton. |
The neoplastic conditions originating from osteoblasts are osteoid osteoma and osteoblastoma, if benign, and osteosarcoma, if malignant. Tumors originating from chondroid cells are chondromas and chondrosarcomas. Those deriving from angioblasts are angiomas and angiosarcomas. Chordoma, a typical tumor of the spine, arises from notochordal remnants. Further tumors originating from osteoclasts, vascular wall fibrous tissue, and mesenchymal neuroangiogenic components are also included.
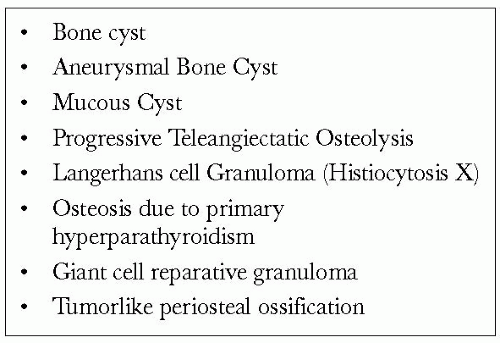 FIGURE 2.2 So called “tumorlike” or “pseudotumoral” bone conditions. |
More conditions, mostly dysplastic or hyperplastic, whose etiology may or may not be known, are the so-called “tumorlike” or “pseudotumoral” lesions (Fig. 2.2), known as such because they may resemble tumors and are often involved in a discussion of differential diagnosis. The most frequent tumorlike condition in the spine is the aneurysmal bone cyst, a hyperplastic reaction of the vascular structures, creating huge cavities filled with membranes and blood.
The classification of soft tissue tumors according to their histogenesis was proposed by Fletcher (12) and approved by the World Health Organization. Soft tumors are not frequent in our series. Involvement of vertebrae by perivertebral soft-tissue tumors is mostly due to tumors originating in the nervous system (neurinoma and its malignant counterpart, schwannoma) and therefore mostly observed in neurosurgical departments. In our series, tumors of fibrous and smooth muscular histogenesis are included. Aggressive fibromatosis, a histologically benign condition generated by fibrous cells, has a tendency for local recurrence and therefore is best treated with en bloc resection. Its malignant counterpart is the fibrosarcoma. Retroperitoneal fibrous and smooth muscular tumors (fibrosarcoma and leiomyosarcoma, respectively) are likely to invade the spine by continuity and pose delicate problems for surgical treatment.
These classifications give little information to the surgeon, who needs elements to understand the biologic behavior. Further, the lack of logically organized paradigm makes it confusing to evaluate the results of treatment for primary spine tumors. Without a common terminology (11),difficulties exist in sharing information and comparing results. The result is that the same procedure (e.g., intralesional excision) is performed for different spine tumors without regard for histology and aggressiveness (19).
The Enneking staging system was set up (10) to grade the aggressiveness of the tumors and to decide on this basis which is the most appropriate surgical margin for any tumor and therefore the extent of surgical en bloc or intralesional excision. A surgical staging system has been proposed for planning the surgical procedure to achieve such margins (6).
avoid high-morbidity surgery when not necessary (for example, in stage 2 benign or in metastatic tumors);
achieve the appropriate margin by correctly performed en bloc resections in selected cases; and
improve the knowledge of these tumors by comparing uniform reports on outcomes of homogeneously treated series,
Enneking Staging System
Enneking (10) proposed in 1980 a classification for bone and soft-tissue tumors that can be adopted for the spine. This classification is based on clinical and laboratory data, imaging, and histology. The combination of all these elements helps to assess the natural history of the disease. Several tumors can occur in different stages, confined inside the compartment of origin or spreading, and the treatment should be pertinent. For each stage, a specific surgery is indicated: intralesional (piecemeal excision or en bloc violating the tumor), marginal (en bloc along the pseudocapsule), wide (outside the pseudocapsule), radical (excision of the entire compartment, if the tumor is intracompartmental).
The terms “vertebrectomy” (removal of all the elements of the vertebra), “corpectomy,” and “somectomy” (removal of the vertebral body) have no significance from an oncologic viewpoint if they are not specified according to the terminology previously mentioned.
All the surgical procedures generally done for a functional purpose (cord decompression, fracture stabilization), with or without partial (piecemeal) removal of the tumor, are called “palliative.” In general, it is intended only to make a diagnosis, decrease pain, and possibly improve function.
The oncologic staging proposed by Enneking (9,10) divides benign tumors into three stages (S1, S2, and S3) and localized (nonmetastatic) malignant tumors into four stages (IA, IB, IIA, and IIB). Two further stages include metastatic high-grade intra- and extracompartmental malignant tumors (IIIA and IIIB, respectively). This classification is based on clinical features, radiographic pattern, CT scan/MRI data, and histologic findings. It was formerly described for long-bone tumors and applied to spinal tumors in some reports (2,3,4,16).
BENIGN TUMORS
The first stage of benign tumors (S1, latent, inactive; Fig. 2.3) includes asymptomatic lesions, bordered by a true capsule, which is usually seen as a sclerotic rim on plain radiograms. These tumors do not grow or grow only very slowly, like hemangiomas or fibrous dysplasia. No treatment is required, unless palliative surgery is needed for decompression or stabilization. Benign tumors, stage 2 (S2, active; Fig. 2.4), grow slowly, causing mild symptoms. Osteoid osteoma, osteoblastoma, and some early giant cell tumors can be observed at this stage. The tumor is bordered by a thin capsule and by a layer of reactive tissue, sometimes found on plain radiograms as an enlargement of the tumor outline. Bone scan is positive. An intralesional excision can be performed with a low rate of recurrence (2). The incidence of recurrences can be reduced further by local adjuvants (cryotherapy, embolization, radiation therapy). The third stage of benign tumors (S3, aggressive; Fig. 2.5
 Place of Bisphosphonates in Spinal Metastases
The Role of Brachytherapy in the Management of Spinal Tumors
Biomechanics of Cement Augmentation in Tumor Treatment
Metastatic Epidural Spinal Cord Compression
Vertebral Augmentation and Radiosurgery in the Treatment of Osteolytic Vertebral Fractures
Intraoperative Radionuclide Localization for Osteoid Osteoma and Osteoblastoma of the Spine
Place of Bisphosphonates in Spinal Metastases
The Role of Brachytherapy in the Management of Spinal Tumors
Biomechanics of Cement Augmentation in Tumor Treatment
Metastatic Epidural Spinal Cord Compression
Vertebral Augmentation and Radiosurgery in the Treatment of Osteolytic Vertebral Fractures
Intraoperative Radionuclide Localization for Osteoid Osteoma and Osteoblastoma of the Spine




Related posts:
Place of Bisphosphonates in Spinal Metastases
The Role of Brachytherapy in the Management of Spinal Tumors
Biomechanics of Cement Augmentation in Tumor Treatment
Metastatic Epidural Spinal Cord Compression
Vertebral Augmentation and Radiosurgery in the Treatment of Osteolytic Vertebral Fractures
Intraoperative Radionuclide Localization for Osteoid Osteoma and Osteoblastoma of the Spine
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
