The clinical features of mood disorders are dimensional, i.e. distributed according to their severity.(1) The categorical approach as manifested in the DSM-IV or ICD-10 does not, however, preclude dimensional descriptions, because in DSM-IV as well as in ICD-10 the categories or diagnoses are essentially defined by minimum and maximum cut-off scores on the symptomatic states.
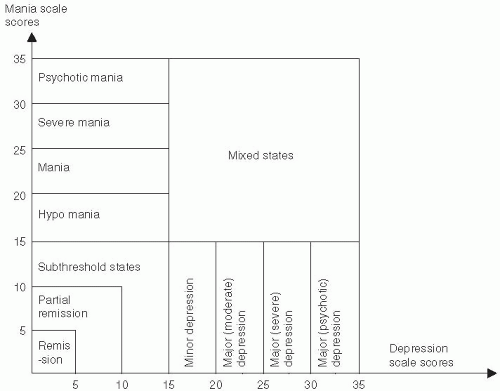
Fig. 4.5.2.1 shows a coordinate system in which the ordinate represents the dimension of manic states and the abscissa the dimension of depressive states. The cut-off scores refer to the standardization of the isometric rating scales for mania and depression.(1,2,3) Jamison(4) has argued that the term ‘bipolar’ perpetuates the notion that: ‘…depression exists rather tidily segregated in its own pole, while mania clusters off neatly and discretely on another. This polarisation of two clinical states flies in the face of everything that we know about the fluctuating nature of manic-depressive illness … and it minimises the importance of mixed manic-depressive states’. William James referred to the stream of consciousness to emphasize its continuity in contrast to its conception as a series of discrete states. However, William James actually confessed that during his own depressive episodes, his mood states,(5) to a large extent, blocked his own stream of consciousness.(6) In the perspective outlined by Jamison,(4) polarity in the clinical world is not two opposites that contradict each other by a logical relationship of juxtaposition. Polarity should rather, as shown in Figs. 4.5.2.1 and 4.5.2.2, be considered at a level of psychological intercorrelations in which clinical mania and depression exist by virtue of each other involving both negative and positive correlations.
Fig. 4.5.2.1 Patient state fluctuations within the spectrum of mood states from the subthreshold states over minor mood states (hypomania or minor depression) to major states (mania/psychotic mania or major depression without or with psychotic symptoms) and to the mixed states.
The symptom rating scales shown in Fig. 4.5.2.1 measure the severity of mania, depression, or mixed states and have a time frame of 3 days. Clinically, this is the minimum for the measurement of the spectrum of mood states ranging from subthreshold states to states of psychotic severity.
Ultrashort states of mood swings are often seen without any reference to mood disorders. In one of Henry James’ masterpieces, The Ambassadors, his autobiographical hero has a tendency towards being introverted in the morning, while in the afternoon and evening he is more extraverted, like a man ‘ … who, elately finding in his pocket more money than usual … ’, though without spending a lot. This 24-h ‘cyclothymia’ between introversion and extraversion displays too mild a symptomatology to be part of a ‘bipolar’ disorder and might be referred to as a temperamental neuroticism. Thus, Eysenck’s original questionnaire for measuring neuroticism included items of being moody without any apparent reason or being inclined to having frequent ups and downs in mood.(7) Neuroticism now seems to include subclinical, temperamental, low, negative affectivity (worrying, gloomy, dysphoric, and hostile).
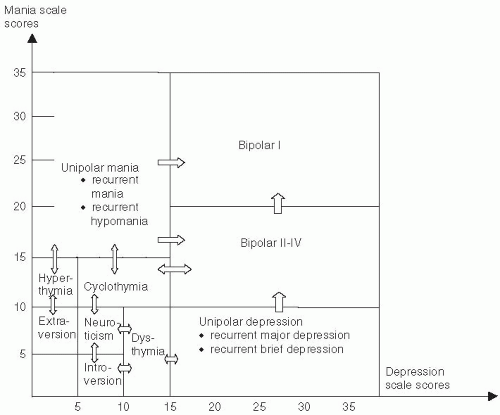
Fig. 4.5.2.2 shows another coordinate system in which the ordinate is representing the dimension of mania severity and the abscissa the dimension of depression severity, but covering the lifelong correlation of the courses of manic and depressive episodes, i.e. the longitudinal diagnosis of mood polarity disorders. While a unipolar course of manic episodes without any depressive episodes is very rare,(8) the course of unipolar depressive episodes without manic episodes is much more frequent. Angst(9) has criticized the DSM-IV definitions of depressive episode disorders (a duration of at least 2 weeks) and of manic episode disorder (a duration of at least 1 week). Thus, Angst has shown that these episode duration criteria are not only too narrow (not sensitive enough), but they also lack empirical evidence (not validated). The spectrum of mood polarity as shown in Fig. 4.5.2.2 is an attempt to refer to the DSM-IV definitions, though modified with reference to Angst.(9) The mood polarity disorder as shown in Fig. 4.5.2.2 is defined by the highest score a given patient has obtained in the coordinate system at any time. Unipolar depression, however, with a score of 10 or less on the mania scale, as shown in Fig. 4.5.2.2, remains a lifelong uncertain diagnosis. Thus, Angst(9) has demonstrated a persistent risk of 1–2 per cent per year of a diagnostic change from unipolar to bipolar disorder.
Fig. 4.5.2.2 Patient state lifetime fluctuations within the spectrum of mood polarity syndromes or disorders from the temperamental neuroticism over minor disorders (dysthymia or cyclothymia) to major unipolar disorders (hypomania/ mania or brief/major depression) and to the various bipolar disorders.
The dimensional approach has been valid also in regard to personality disorder. As discussed by Angst,(9) only around 15 per cent of the general population seem to report no lifelong personality disorders, and he therefore calls these persons ‘supernaturals’. Thus, nearly everyone has some kind of personality disorder, and within the spectrum of mood personality disorders, extraversion, introversion, neuroticism, hyperthymia, dysthymia, and cyclothymia are to be considered subthreshold disorders as shown in Fig. 4.5.2.2.
It has recently been argued that when taking into account both the subthreshold levels of symptoms and the short states of 2–3 days’ duration rather than the whole DSM-IV episodes, there appears to be a linear correlation between mania and depression in the course of illness in many patients with mood disorders.(10)
The depressive episode: duration and severity
Table 4.5.2.1 shows the DSM-IV and ICD-10 depressive symptoms for the diagnosis of major depression, which to a large extent covers the rating scale dimension in Fig. 4.5.2.1. Thus, the individual symptoms should be present most of the day and nearly every day during an episode. Kendler and Gardner(11) have shown that the risk of developing a new major depressive episode (i.e. of a duration of 14 days or more) is as high for patients with major depressive symptoms lasting from 5 to 13 days as for patients with symptoms lasting from 14 to 59 days.
The study by Kendler and Gardner(11) has also demonstrated that patients with a subthreshold quantity of depressive symptoms (i.e. just below five out of the nine DSM-IV symptoms listed in Table 4.5.2.1 or minor depression in Fig. 4.5.2.1) had the same risk of developing a new major depressive episode as patients fulfilling the symptomatic criteria of major depression. It has been shown that approximately 50 per cent of the patients fulfilling the ICD-10 category of mild depression also fulfil the criteria for DSM-IV major depression.
To illustrate how a major depressive episode often develops on a continuum of depressive symptoms from the first prodromes of decreased positive well-being (introversion) to the major depressive episode, a layman’s description is shown in Box 4.5.2.1. These autobiographical notes of the late William Styron (1925–2006) describe his first episode of depression at the age of 60.(12) As indicated, the symptom of anxiety (not included in DSM-IV or ICD-10) is a very important symptom of major depression from its very onset. When suicidal impulses developed, he was admitted to Yale New Hospital.
Table 4.5.2.1 Depression symptoms as included in DSM-IV and ICD-10
Symptoms of depression
DSM-IV
ICD-10
1 Depressed mood most of the day, nearly every day
+
+
2 Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day
+
+
3 Loss of energy or fatigue nearly every day
+
+
4 Loss of confidence or self-esteem
−
+
5 Unreasonable feelings of self-reproach or excessive or inappropriate guilt, nearly every day
+
+
6 Recurrent thoughts of death or suicide, or any suicidal behaviour
+
+
7 Diminished ability to think or concentrate, or indecisiveness, nearly every day
+
+
8 Psychomotor agitation or retardation nearly every day
+
+
9 Insomnia or hypersomnia nearly every day
+
+
10 Change in appetite (decrease or increase with corresponding weight change)
+
+
+ indicates that the symptom is included; – indicates that the symptom is not included.
Only gold members can continue reading. Log In or Register to continue
 Prevention of mental disorder in childhood and other public health issues
Prevention of mental disorder in childhood and other public health issues



