Clinical Neuropsychological Testing
The neuropsychological examination has a valuable place in diagnosing and treating behavioral syndromes that are associated with medical, psychological, and psychiatric conditions. Clinical neuropsychology is a specialty within psychology that examines the relationship between behavior and brain functioning in the realms of cognitive, motor, sensory, and emotional functioning. Neuropsychologists integrate the medical and psychosocial history with the chief complaint and pattern of performance on neuropsychological procedures. Such analysis determines whether results are consistent with a particular area of brain damage or a particular diagnosis.
The neuropsychological examination systematically assesses functioning in the realm of attention and concentration, memory, language, spatial skills, sensory and motor abilities, as well as executive functioning and emotional status. Assessment instruments are standardized against normal control subjects. This ensures that test administration and scoring are invariant across time and examiners. Resulting data show whether the test is valid and reliable. The aim of neuropsychological tests is to achieve quantifiable and reproducible results that can be compared with the test scores of normal people of comparable age and demographic background.
There are two types of tests: objective and projective. Objective tests are typically pencil-and-paper tests based on specific items and questions. They yield numerical scores and profiles subject to mathematical and statistical analysis. Projective tests present stimuli whose meaning is not immediately obvious. Projective tests presumably have no right or wrong answers. Those being tested impute meanings to the stimulus, based on psychological and emotional factors.
The student should be familiar with the types of neuropsychological assessment tests that are available, how they are administered, and their indications for use.
Helpful Hints
The student should know the following terms, theoreticians, and concepts.
abstract reasoning
accurate profile
battery tests
behavioral flexibility
bell-shaped curve
Bender Visual Motor Gestalt Test
catastrophic reaction
clang association
classification of intelligence
coping phase
dressing apraxia
dysgraphia
dyslexia
EEG abnormalities
Eysenck personality inventory
fluency
Gestalt psychology
Halstead-Reitan
House-Tree-Person Test
individual and group tests
intelligence quotient (IQ)
learning disability
left versus right hemisphere disease
Luria-Nebraska Neuropsychological Battery (LNNB)
manual dexterity
maturational levels
memory: immediate, recent, recent past, remote
mental age
mental status cognitive tasks
MMPI
motivational aspects of behavior
neuropsychiatric tests
objective tests
organic dysfunction
performance subtests
perseveration
personality testing
primary assets and weaknesses
projective tests
psychodynamic formulations
Raven’s Progressive Matrices
reaction times
recall phase
response sets
Rorschach Test
scatter pattern
Shipley Abstraction Test
Stanford-Binet
stimulus words
TAT
temporal orientation
verbal subtests
visual-object agnosia
WAIS
WISC
word-association technique
Questions
Directions
Each question or incomplete statement below is followed by five suggested responses or completions. Select the one that is best in each case.
4.1. For the general population, an intelligence quotient (IQ) of 100 corresponds to intellectual ability in the
A. 20th percentile
B. 25th percentile
C. 40th percentile
D. 50th percentile
E. 65th percentile
View Answer
4.1. The answer is D
An intelligence quotient (IQ) of 100 corresponds to the 50th percentile in intellectual ability for the general population. Modern psychological testing began in the first decade of the 20th century when Alfred Binet (1857–1911), a French psychologist, developed the first intelligence scale to identify mentally challenged youngsters. The Stanford-Binet Scale is a standardized intelligence test assessing both cognitive ability and intelligence from age 2 onward. It is useful for determining the presence of a learning disability, developmental delay, or brain damage in people with neurological insults. Its components include general intelligence, visuospatial processing, quantitative reasoning, fluid reasoning, knowledge, and memory.
4.2. Neuropsychological deficits associated with left hemispheric damage include all of the following except
A. limb apraxia
B. visuospatial deficits
C. finger agnosia
D. aphasia
E. right–left disorientation
View Answer
4.2. The answer is B
Many functions are mediated by both the right and left cerebral hemispheres. However, important qualitative differences between the two hemispheres can be demonstrated by the presence of lateralized brain injury. Various cognitive skills that have been linked to the left or right hemisphere in right-handed people are listed in Table 4.1. Although language is the most obvious area that is largely controlled by the left hemisphere (with injuries leading to aphasias), the left hemisphere is also generally considered to be dominant for limb praxis (i.e., performing complex movements, such as brushing teeth, commanding, or imitation). The left hemisphere has been associated with a cluster of deficits identified as Gerstmann syndrome (i.e., finger agnosia, dyscalculia, dysgraphia, and right–left disorientation). In contrast, the right hemisphere is thought to play a more important role in controlling visuospatial abilities and hemispatial attention, which are associated with the clinical presentations of constructional apraxia and neglect, respectively.
Although lateralized deficits such as these are typically characterized in terms of damage to the right or left hemisphere, it is important to keep in mind that the patient’s performance can also be characterized in terms of preserved brain functions. In other words, it is the intact brain tissue that drives many behavioral responses following injury to the brain.
Table 4.1 Selected Neuropsychological Deficits Associated with Left or Right Hemisphere Damage | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
4.3. Neuropsychological referrals are made for
A. establishing a baseline of performance
B. diagnostic purposes
C. ascertaining brain impairment
D. planning for rehabilitation
E. all of the above
View Answer
4.3. The answer is E (all)
Most neuropsychological referrals are made for diagnostic purposes, to ascertain if brain impairment is present, or to differentiate among neurological or psychiatric disorders. Other important uses of testing include establishing a baseline of performance for assessing future change and planning for rehabilitation and management of behaviors affected by brain impairment. The specific methods of neuropsychological assessment reflect the individual’s unique presentation of symptoms and complaints, history and development, the perspective of the neuropsychologist, and the reason for referral.
A common referral issue involves documentation of level of functioning for a variety of purposes, including assessment of change or competence, especially in the presence of diagnoses such as dementia, stroke, and head injury.
4.4. True statements about projective personality tests include
A. They often focus on latent or unconscious aspects of personality.
B. The variety of responses is limited.
C. They tend to be more direct and structural than objective personality tests.
D. Instructions are usually specific.
E. None of the above
View Answer
4.4. The answer is A
Projective personality tests, in contrast to objective personality instruments, are more indirect and unstructured. Unlike objective tests, in which the patient may simply mark “true” or “false” to given questions, the variety of responses to projective personality tests is almost unlimited. Instructions are usually general, allowing the patient’s fantasies to be expressed. Patients generally do not know how their responses will be scored or analyzed, making it difficult to obtain a desired result. Projective tests typically do not measure one particular personality characteristic such as type A personality (i.e., narrow-band measurement) but instead are designed to assess a personality as a whole (i.e., broad-band measurement).
Projective tests often focus on latent or unconscious aspects of personality. Obviously, psychologists and others differ in the degree to which they rely on unconscious information. In many projective techniques, patients are simply shown a picture of something and asked to tell what the picture reminds them of. Projective techniques assume that when presented with an ambiguous stimulus such as an inkblot, for which there are an almost unlimited number of responses, the patients’ responses will reflect fundamental aspects of their personalities. The ambiguous stimulus is a sort of screen on which individuals project their own needs, thoughts, or conflicts. In particular, a schizophrenic patient’s responses will often reflect a rather bizarre, idiosyncratic view of the world. Hundreds of different projective techniques have been developed—most of which are not used widely today.
4.5. After taking the Wechsler Adult Intelligence Scale (WAIS), a patient was found to have poor concentration and attention. Select the WAIS subtest that most likely screened the patient for these symptoms.
A. block design
B. comprehension
C. arithmetic
D. digit symbol
E. picture completion
View Answer
4.5. The answer is C
The arithmetic subtest uses simple arithmetic tasks to assess attention and concentration. The block design subtest requires a subject to arrange a series of pictures to tell a story. This process tests performance and cognitive styles. The digit symbol subtest requires a subject to match digits and symbols in as little time as possible, as a test of performance. The comprehension subtest reveals a subject’s ability to adhere to social consequences and to understand social judgments when the subject answers questions about how people should behave. On the picture completion subtest, a subject must complete a picture with a missing part. Visuospatial defects appear when errors are made on this picture completion procedure.
4.6. The Bender Visual Motor Gestalt Test is administered to assess
A. maturation levels in children
B. organic dysfunction
C. loss of function
D. visual and motor coordination
E. all of the above
View Answer
4.6. The answer is E (all)
The Bender Visual Motor Gestalt Test, devised by the American neuropsychiatrist Lauretta Bender in 1938, is a technique that consists of nine figures that are copied by the subject (Fig. 4.1). It is administered as a means of evaluating maturation levels in children and organic dysfunction. Its chief applications are to determine retardation, loss of function, and organic brain defects in children and adults. The designs are presented one at a time to the subject, who is asked to copy them onto a sheet of paper. The subject is then asked to copy the designs from memory (Figs. 4.2 and 4.3); thus, the Bender designs can be used as a test of both visual and motor coordination and immediate visual memory.
4.7. Which is not true of the Wisconsin Card Sorting Test?
A. It assesses abstract reasoning
B. It assesses parietal lobe dysfunction
C. The patient is told during testing whether their responses are correct or incorrect
D. The examiner records the number of trials required to achieve ten consecutive correct responses
E. The examiner changes the principle of sorting when the task is mastered
View Answer
4.7. The answer is B
Persons with damage to the frontal lobes or to the caudate nucleus, and some patients with schizophrenia, give abnormal responses to the Wisconsin Card Sorting Test (WCST). It does not address parietal lobe damage. This test assesses abstract reasoning and flexibility in problem solving. Stimulus cards are presented to patients to sort into groups according to a principle established by the examiner but unknown to the patient. As the patient sorts the cards, he or she is told whether the responses are correct or incorrect. The number of trials required to achieve ten consecutive correct responses is recorded. When or if the patient has mastered the task, the examiner changes the principle of sorting, and the number of trials required to achieve correct sorting is again recorded.
4.8. In the Wechsler Adult Intelligence Scale (WAIS),
A. digit span is a subtest of the verbal component of the test
B. its latest revision is designed for persons aged 16 to 60
C. mental retardation corresponds to the lowest 1% of the population
D. the average range of IQ is 100 to 120
E. the verbal scale is more sensitive to normal aging
View Answer




4.8. The answer is A
The Wechsler Adult Intelligence Scale (WAIS) comprises 11 subtests made up of six verbal (information, comprehension, arithmetic, similarities, digit span, vocabulary), and five performance (picture completion, block design, picture arrangement, object assembly, digit symbol) subtests, which yield a verbal IQ, a performance IQ, and a combined full-scale IQ. The latest edition, the WAIS-III, is designed for persons 16 to 89 years of age. There are also scales for children ages 4 to 6.5 and 5 through 15. The average or normal range of IQ is 90 to 110; IQ scores of at least 120 are considered superior. Mental retardation, defined as IQ below 70, corresponds to the lowest 2.2 percent of the population; 2 of every 100 people have IQ scores consistent with mental deficiency. The performance scale is more sensitive to normal aging than the verbal scale, which is more sensitive to education.
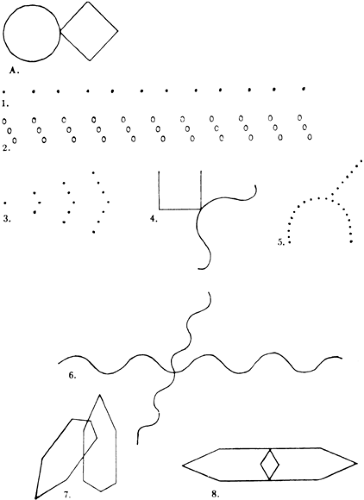 Figure 4.1 Test figures from the Bender Visual Motor Gestalt Test, adapted from Max Wertheimer. (Reprinted with permission from Bender L. A Visual Motor Gestalt Test and Its Clinical Use. New York: American Orthopsychiatric Association; 1938:33.) |
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
