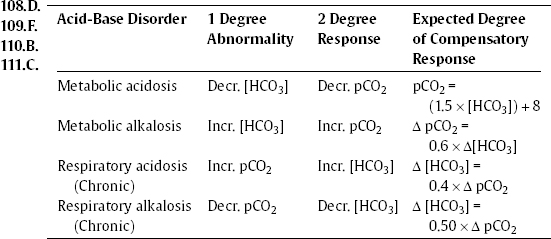
Chapter 14 Clinical Skills/ Critical Care 1.E. For questions 1–6 see Barash pp. 749–750. 2.D. 3.A. 4.E. 5.F. 6.B. 7.A CNBR p. 280. 8.A. Clin PR pp. 463–467. Adenosine at an initial dose of 6 mg over 1 to 3 seconds, followed by a repeat of 12 mg in 1 to 2 minutes prn, is the initial drug of choice. If lidocaine is ineffective, procainamide at a dose of 20 to 30 mg/min for a maximum of 17 mg/kg is given. 9.A. Sch p. 459. Neurologic involvement does not develop in the absence of pulmonary abnormalities unless there is the rare event of a paradoxical embolus through a patent foramen ovale. 10.A. Har p. 737. Transfusion-associated graft-versus-host disease may result if viable lymphocytes in blood are not irradiated. 11.A . Sch p. 96. 12.D. For questions 12–14 see Y p. 1196. 13.A. 14.A. 15.B. Har pp. 351, 663. 17.A. Har pp. 427–428. Trimethoprim sulfamethoxazole (Bactrim) increases the effect of Coumadin by decreasing clearance. Barbiturates and rifampim accelerate Coumadin clearance by inducing hepatic metabolizing enzymes, and cimetidine inhibits its oxidative metabolism. 18.A. Har p. 1326. Metabolic side effects of thiazide diuretics include hypokalemia from renal potassium loss, hyperuricemia from uric acid retention, carbohydrate intolerance, and hyperlipidemia. 19.A. Har pp. 427, 2364–2365. Carbamazepine (Tegretol) decreases plasma levels of phenytoin (Dilantin). 20.D. Sch p. 1017. Nonspecific sinus tachycardia (ST) and T wave changes occur in 66% of patients. 21.B. Clin PR pp. 184–185. 22.D. Sch pp. 62–63. 23.C. Har p. 1537. 24.C. For questions 24–27 see G&G pp. 1534–1536. Aspirin inactivates cyclooxy- 25.A. genase, the enzyme that produces the precursor of thromboxane A2. Ticlodipine 26.D. and clopidogrel are thienopyridines that block the Gi-coupled platelet 27.B. adenosine diphosphate (ADP) receptor. They are thought to be prodrugs requiring conversion to the active metabolite. Thrombocytopenia and leukopenia occur less commonly with clopidogrel. Reopro and Integrilin are the inhibitors of glycoprotein IIb/IIIa receptor, but the former is the Fab fragment of a humanized monoclonal antibody against the receptor, and the latter is a cyclic peptide inhibitor of the arginine-glycine-aspartate (RGD) binding site on the receptor. 28.A. Har p. 754. 29.D. West p. 65. 30.A. Sch pp. 26–33. Hyperglycemia, not hypoglycemia, is one of the metabolic responses to trauma. 31.C. Har p. 359. Deficiency of factors II, V, or X causes prolonged PT and PTT. A deficiency of factor XII causes a prolonged PTT but no clinical bleeding. 32.B. For questions 32–37 see Har pp. 359–360, 751–754. A deficiency of factor V also 33.B. results in prolonged PT and PTT. 34.C. 35.D. 36.C. 37.E. 38.E. For questions 38–45 see Har pp. 359–360, 751–754. 39.A. 40.D. 41.A. 42.B. 43.B. 44.C. 45.F. 46.C. For questions 46–52 see Har pp. 285–291. Respiratory alkalosis is the earliest 47.B. abnormality and may be the only acid-base disorder in some patients with 48.E. salicylate overdose. Production of a mixture of endogenous acids, from a 49.D. metabolic block, may later lead to metabolic acidosis. 50.A. 51.C. 52.C. 53.D. Sch p. 493, Table 12-2. 54.C. For questions 54–60 see Har pp. 2184–2185, 2187. MEN type I (Wermer’s 55.A. syndrome) is characterized by parathyroid, pancreatic, and pituitary tumors, 56.A. most commonly. MEN type IIA (Sipple’s syndrome) is characterized by medullary 57.B. thyroid carcinoma, pheochromocytoma, mucosal and gastrointestinal neuromas, 58.B. and marfanoid features. Rarely, pheochromocytomas may be seen in MEN type I. 59.D. 60.D. 61.A. Har pp. 2095–2096. In the absence of associated disorders, edema is characteristically absent. 62.C. Har p. 1452, West pp. 46–47. 63.D. For questions 63–68 see Har pp. 1269–1375. 64.E. 65.C. 66.B. 67.A. 68.D. 69.E. Har pp. 92, 94. Barash pp. 521–529. Succinylcholine can precipitate malignant hyperthermia. 70.B. Har pp. 926–927. Oral vancomycin is also effective in the treatment of this infection. 71.A. For questions 71–73 see Sch pp. 159, 684. 72.C. 73.D. 74.E. Apuzzo pp. 135–136. 75.A. Apuzzo p. 132. 76.A. Apuzzo p. 136. 77.C. For questions 77–81 see Clin PR pp. 398, 529–530. 78.A. 79.B. 80.D. 81.B. 82.E. Har p. 2462. Gram-negative bacilli and group B streptococci are the most common causes of neonatal meningitis. 83.D. G&G pp. 889–890, 924. Cyanide is reduced to thiocyanate in the liver, and the thiocyanate is then excreted in the urine. 84.E. G&G p. 228. Isoproterenol acts almost exclusively on beta receptors. It increases (or leaves unchanged) systolic blood pressure and decreases diastolic blood pressure, and mean arterial pressure typically falls. It also decreases peripheral vascular resistance and relaxes smooth muscle. 85.A. Har pp. 682–683. Splenectomy for hereditary spherocytosis leads to normal or near normal red blood cell (RBC) survival. It does not correct the RBC deficit and should be performed after age 4, when the risk of severe infections is low. Rare relapses have been reported. 86.A. For questions 86–92 see Sch 5 pp. 318–320. 87.E. 88.B. 89.D. 90.B. 91.B. 92.D. 93.A. Har p. 1661. Intravenous secretin increases serum gastrin in patients with a gastrinoma. 94.C. For questions 94–99 see Har pp. 1602–1604. Hyperkalemia is found in renal 95.D. tubular acidosis (RTA) type 4. Nephrocalcinosis is rare in RTA type 2, and the 96.A. urine pH is les than 5.5 in this type. 97.A. 98.B. 99.C. 100.C. Clin PR p. 177. 101.B. Barash p. 766. End-tidal pCO2 decreases with venous air embolism. 102.D. Barash p. 766. The most sensitive is transesophageal echocardiography, the most sensitive noninvasive monitor is the precordial Doppler. 103.C. Har p. 1267. Transmural ischemia may lead to ST elevation in the electrocardiogram (EKG). 104.A. Har p. 2068. Occasionally, in patients with hypothyroidism of pituitary or hypothalamic origin, serum thyroid-stimulating hormone (TSH) concentrations may be slightly increased rather than decreased if the form of TSH secreted is immunoactive but not bioactive. 105.A. Har p. 282. Calcium gluconate infusion is useful for cardiotoxicity, but it does not reduce serum potassium. 106.E. For questions 106–111 see Clin PR pp. 163–164. Formulas helpful in the 107.A. calculation of simple acid-base disturbances are listed below:
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


