♦ Preoperative
Imaging
- Computed tomography: isodense to hyperdense round cyst in the third ventricle with or without obstructive hydrocephalus
- Magnetic resonance imaging (MRI): cyst of variable intensity, usually hyperintense on T1; in the third ventricle; may enhance with contrast; size of ventricles is important factor in determining approach; assess cortical veins on contrast images or magnetic resonance venography if planning an interhemispheric transcallosal approach
Surgical Approach
- Choice based on ventricular size, surgeon experience, and goals of operation
- Transcortical
- Advantages: direct route to lateral ventricle, especially accessible if ventricles are dilated; ability to widen cortical opening to minimize frontal lobe retraction; if ventriculostomy already in place, may follow tract down to ventricle
- Disadvantages: substantial amount of frontal lobe traversed, especially if ventricles are small; postoperative porencephalic cyst in the frontal lobe with a potential persistent cerebrospinal fluid (CSF) tract
- Advantages: direct route to lateral ventricle, especially accessible if ventricles are dilated; ability to widen cortical opening to minimize frontal lobe retraction; if ventriculostomy already in place, may follow tract down to ventricle
- Transcallosal
- Advantages: relatively minimal dissection through white matter compared to transcortical approach; straight trajectory down to third ventricle
- Disadvantages: need to have complete or partial exposure of the sagittal sinus with potential for bleeding; risk of sinus occlusion with retraction; exposure may be restricted by bridging veins from frontal lobe into sagittal sinus
- Advantages: relatively minimal dissection through white matter compared to transcortical approach; straight trajectory down to third ventricle
- Endoscopic
- Advantages: minimally invasive with minimized incision, blood loss, and hospital stay; minimal retraction on the frontal lobe
- Disadvantages: difficulty in obtaining complete excision of cyst wall if adhered to surrounding structures; difficult to open roof of third ventricle if foramen needs to be enlarged; access to small ventricles is difficult without stereotactic navigation
- Advantages: minimally invasive with minimized incision, blood loss, and hospital stay; minimal retraction on the frontal lobe
- Mayfield head holder
- Craniotomy tray with microdissectors and micromirror
- High-speed drill
- Retractor system (Budde halo, Greenberg retractor, or Yasargil)
- Bipolar cautery
Endoscopic Equipment
- Rigid endoscope
- Endoscopic biopsy cup forceps, suction, bipolar and/or monopolar cautery, microscissors
Operating Room Set-up
- Frameless stereotactic navigation if needed for ventricular access
- Ultrasound if needed for guidance toward ventricle in transcortical approach
- Microscope
- Sitting stools if needed
- Endoscopy: video monitors at foot of bed
Anesthetic Issues
- Preoperative antibiotics within 30 min of incision
- Intravenous steroids (dexamethasone)
- Arterial line
- Precordial Doppler for transcallosal approach
♦ Intraoperative
Transcortical
- Nondominant side is preferred
- Position supine with head turned to left and flexed to elevate right frontal region
- Shave hair, plan linear incision anterior to the coronal suture
- Alternative incision is U-shaped flap that flaps laterally
- If ventriculostomy already inserted, will have to exclude exit site from operative field
- Bone flap straddles the coronal suture with two thirds of it anterior and one third posterior to the suture; incorporates the ventriculostomy if present
- Dural opening in cruciate fashion
- Enter through gyrus or sulcus toward ventricle
- Pathway toward ventricle may be guided by a ventriculostomy already present, a newly passed ventricular catheter, or ultrasound
- Insert retractor system after lateral ventricle opened. Bring in the microscope.
- Identify the septal and thalamostriate veins, choroid plexus, fornix, foramen of Monro, and cyst capsule
- Dissect adhesions to capsule where visible
- Lay cotton patties around cyst and on ventricular wall prior to opening the cyst to prevent leakage of contents throughout ventricular system, which may cause chemical meningitis
- Bipolar cautery to cyst capsule, capsule opened sharply, and cyst contents aspirated
- Continue to dissect cyst wall free from roof of third ventricle, tela choroidea, and choroid plexus
- Coagulate the anterior choroid plexus in the lateral ventricle
- Third ventricle may be opened through the tela choroidea which is visible after coagulating the choroid plexus
- Third ventricle may need to be further opened by ligation of thalamostriate vein
- After excision, inspect roof of third ventricle with mirror or flexible endoscope
- Fenestrate the septum pellucidum in case of shunt requirement in the future
- Option of pial sutures to close cortical opening to prevent excess egress of CSF
- Need watertight dural closure
- Bipolar cautery to cyst capsule, capsule opened sharply, and cyst contents aspirated
Transcallosal
- Nondominant side is preferred
- Position patient supine with head flexed and neutral rotation or turned slightly to the left
- Modified bicoronal incision slightly anterior to the coronal suture from right temporal region to left superior temporal line
- Plan craniotomy that straddles the coronal suture with two thirds anterior to it and one third posterior
- Craniotomy also extends over superior sagittal sinus
- Burr holes on both sides of the midline to allow for complete freeing of the bone from the sinus. Ensure that cuts adjacent to sagittal sinus are performed last.
- Place Surgicel and Gelfoam with thrombin in strips along sagittal sinus to control bleeding
- Dural incision with a flap toward the sinus
- Suture the dural flap to the other side, but without too much tension to avoid occlusion of the superior sagittal sinus
- Identify bridging veins and dissect arachnoid around them if needed to mobilize them. Veins anterior to the coronal suture can be coagulated and divided in order to provide wider corridor of dissection.
- Begin frontal lobe retraction, allow CSF to be released from interhemispheric fissure for gradual relaxation of the brain
- Place retractors on frontal lobe and on falx
- Identify the corpus callosum and pericallosal arteries, which are retracted laterally
- Opening of 2 to 3 cm into the corpus callosum
- Identify which lateral ventricle has been entered by locating landmarks, such as the septal vein, choroid plexus, and foramen of Monro
- Microdissection of the colloid cyst as described above
- Need watertight dural closure
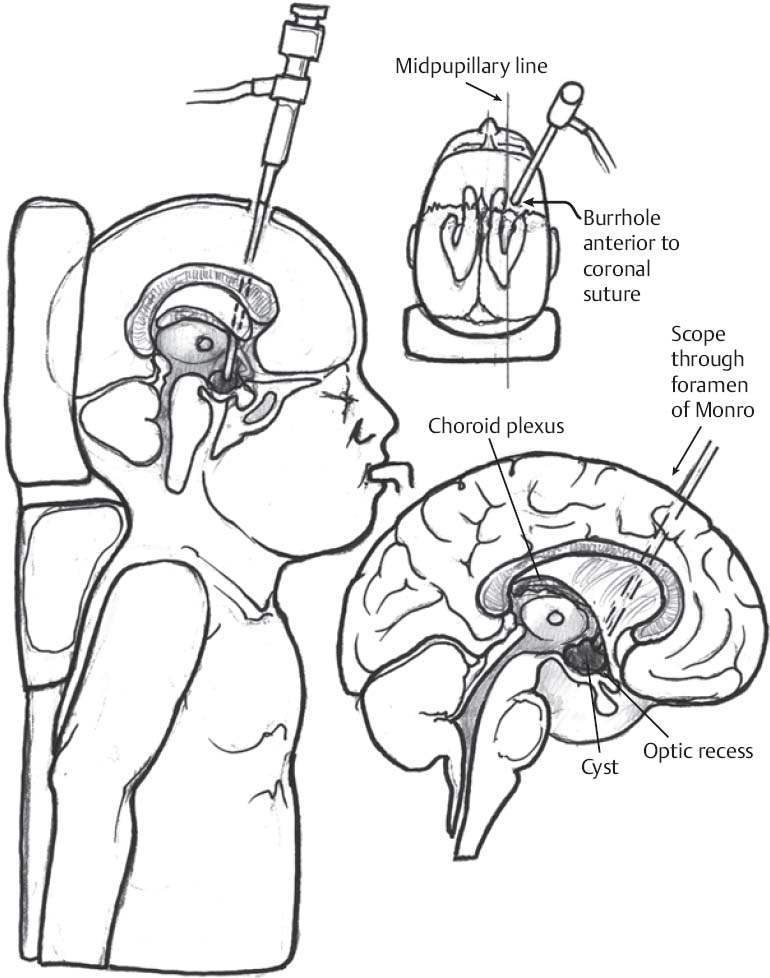
Endoscopic (Fig. 52.1)
- Position patient supine with head flexed 30 degrees on doughnut or cerebellar headrest with small roll underneath shoulders
- Frameless stereotactic navigation: head affixed in Mayfield holder, registration, and planning of burr hole and trajectory
Only gold members can continue reading. Log In or Register to continue







