The topic of consciousness is relevant to psychogenic movement disorders, both because of close conceptual links between consciousness and volition, and because our understanding of psychogenesis is intertwined with our understanding of consciousness. The etymologic root of consciousness in Latin implied the sharing of knowledge. In colloquial English, the term can refer either to wakefulness or to awareness. Self-consciousness can refer to self-detection, self-recognition, the “awareness of awareness” and self-knowledge broadly construed. Over the 20th century, work in neurology and neuroscience has greatly extended our knowledge of the neural basis of both wakefulness and awareness. Research contrasting brain activity in conscious and unconscious states suggests that several factors influence the likelihood that local processing will give rise to awareness; these factors include the amplitude and duration of processing, the degree of synchronization of neuronal activity, the brain regions involved, and the details of their connectivity. There is a growing consensus that the neurology of awareness involves the operation of a “global workspace” which allows local activity to be broadcast widely through the brain. Whether theories framed in these terms can solve the “hard problem” of consciousness—why neural processing should cause subjective awareness at all—is controversial. Work on a variety of forms of disordered movement and action provide potential analogies for psychogenic movement disorders: Several types and levels of explanation are likely to be required to understand these fully.
WHY IS CONSCIOUSNESS RELEVANT TO PSYCHOGENIC MOVEMENT DISORDERS?
A chapter devoted to the problem of consciousness may seem out of place in a volume concerned with movement disorders. However, it soon became clear at the meeting which this book commemorates that any attempt to make sense of psychogenic movement disorders (PMDs) compels one to take account of consciousness. In this introductory section I shall outline two reasons why this should be so, before reviewing relevant aspects of the contemporary state of consciousness science. The chapter will conclude by exploring themes and models from the study of awareness which may help us to understand PMDs. Although I will not explore the historical background here, I note in passing that the history of thinking about consciousness over the past 200 years has been intertwined with thinking about PMDs; Charcot’s writings on hypnosis, Janet’s concept of dissociation, and Freud’s views on the unconscious all owed much to their encounters with these puzzling disorders.
The first link between consciousness and PMDs goes by way of the concept of will or volition. Roughly speaking, willed or volitional acts are those which flow, or seem to flow, from conscious intentions. Conscious intentions, in turn, are those of which we are aware, which we are prepared to acknowledge as our own, or which were, or might have been, the outcome of a process of reflection. Will is therefore, in a sense, the active face of consciousness, the expression of consciousness in action. Now the will is clearly relevant to PMDs, for the following reason: PMDs are typically disorders which appear at first glance to resemble neurologically more straightforward organic disorders, like Parkinson disease or paralysis due to stroke, but which on further assessment turn out to (i) have no basis in pathologically defined neurologic disease and (ii) have a plausible psychological explanation of some kind. That is, they turn out to resemble willed or volitional actions at least as closely as they resemble orthodox neurologic disorders; it is as if the patient is “acting” the role of a patient with parkinsonian tremor or stroke-induced paralysis. Yet, by and large, patients with PMDs deny that they are willing or consciously producing their symptoms— and we are, by and large, inclined to believe them (I shall return to the difficult issue of malingering). This state of affairs obliges us to come up with an explanation of how actions, which closely resemble those that we will, can occur in the absence of normal volition, by way of unconscious or subconscious routes which somehow bypass awareness. This train of thought makes it clear that if we are to understand PMDs, we will have to take an interest in both the concept and the neurology of consciousness, and of its counterpart, volition.
The second link between consciousness and PMDs is fundamental. It relates to a dilemma which surfaced with great regularity at our meeting, particularly in connection with our choice of terminology for the disorders under discussion: the relationship between the body and the mind. The central problem of consciousness, much discussed in recent work in which it is sometimes termed the “hard problem,” is how the 1011 intricately organized neurons within our brains give rise to our mental lives: to sensations, emotions, intentions, or, in a word, to our experience. This is an ancient problem in modern disguise—the problem of how mind and body, psyche or soma, the functional and the organic are related. These dichotomies are deeply entrenched in our everyday thought, and we find them seductive. We use them to carve up intellectual and professional territories. We want a clear answer to the question of whether a movement disorder is organic or psychogenic: If organic, it belongs to the neurologist, if psychogenic, to the psychiatrist. This is a pragmatic approach with which most medical readers will be thoroughly familiar. Yet, in our reflective moments, few if any of us believe that these apparent oppositions—mind versus body and the like—are anything of the kind. All our scientific knowledge of experience, behavior, and the brain insists that the mind is a function of the brain, psyche a function of soma, the functional a vital aspect of the living organism. We are, in other words, saddled with a set of time-honored distinctions in which we do not believe, yet cannot do without; in time, this will have to change.
Imagine for a moment that it has changed. Accept, as I think most of us believe, that all illness—indeed all normal human behavior—has both a physiologic and a psychological dimension. We would surely still need some way of distinguishing the kinds of movement disorders under consideration here from their organic cousins, for example, psychogenic tremor from the tremor of Parkinson disease. If a biopsychosocial (or psychobiologic) approach is appropriate to both, then what’s the difference between them? I suggest that, first, to reiterate the argument of the previous paragraph, this approach reminds us that the differences between these two kinds of disorders are less fundamental than we normally tend to suppose. But second, accepting that there are indeed some important differences, they lie in two main areas: (i) most PMDs have the potential to be brought under voluntary control to a greater extent than most orthodox neurologic movement disorders, although this difference is one of degree rather than kind, and (ii) the etiologic explanation of PMDs will mostly be at a different level from the etiologic explanation of organic disorders. The explanation of the latter will appeal largely to a chain of neuropathologic events, while the explanation of the former will appeal largely to life events, personality, and mood; different kinds of stories most readily make sense of the different classes of disorder. But once again the difference is of degree, not kind, and there will be numerous points of contact between physical and psychological factors in both organic and functional movement disorders.
WHAT DO WE MEAN BY “CONSCIOUSNESS”?
The word “consciousness” originates from the elision of two Latin words: cum, meaning “with,” and scio, meaning “know” (1). To be conscious of information in the original Latin sense was to share the knowledge of it with another person: The knowledge in question was often secret or shameful, the kind one would share with a co-conspirator. But, of course, knowledge that can be shared literally with another person can also be shared metaphorically with oneself, as in this 17th-century example: “I am conscious to myself of many failings.” As the use of the term evolved in the English language, it weakened, so that being conscious sometimes meant simply “knowing.” But the original sense of shared knowledge lives on in the background of our thoughts, coloring our use of consciousness. As we shall see, it still resonates in current scientific theories of consciousness.
In contemporary colloquial and scientific use, consciousness is used in two key senses: wakefulness and awareness (2,3). The first is relatively straightforward. In emergency rooms all over the world it is important to establish whether patients are or are not conscious in the sense of being able to perceive and respond to events around them in the well-integrated fashion which characterizes a normal state of alertness. The use of objective criteria, such as those brought to bear by the Glasgow Coma Scale (GCS)—which considers eye opening, and verbal and motor behavior—generally allows an accurate assessment of consciousness in this first sense. Such criteria allow us to distinguish both degrees of consciousness, for example, GCS 10/15 versus 15/15, or drowsy versus wide awake, and states of consciousness, for example, wakefulness versus sleep or coma.
The second sense of consciousness, awareness, is less obviously exhausted by objective descriptors and much more controversial in consciousness science. However, it is clear enough that while we are conscious in the first sense I have distinguished, we are normally conscious of something; awareness refers to the contents of consciousness. Numerous authors (4, 5, 6, 7, 8, 9, 10) have drawn attention to features of these contents which most agree call out for explanation: The contents of consciousness are stable over short periods, of a few hundred milliseconds, but typically changeful over longer periods. They have a limited capacity at any one time, often combining a sharply focused background with a less highly specified background, but over time they can range right across the spectrum of our cognitive capacities. We can be conscious of sensations, thoughts, memories, emotions, plans, and so on, and our awareness from moment to moment often combines elements from several of these sources. Awareness of the present is usually connected with awareness of the past by means of memory. Our awareness is perspectival, always afforded by a particular, necessarily limited, point of view. Our capacity for awareness is fundamental to the value we place upon our lives; most of us would not wish to be kept alive if it were clear that we had lost this capacity forever. The distinction between wakefulness and awareness is exploited in the familiar description of the vegetative state as one of wakefulness without awareness, a condition in which some objective signs of wakefulness—eye opening and a (very limited) degree of responsiveness to environmental stimuli— are present, but there is no evidence of any sophisticated form of awareness, of any “inner life.”
Discussions of consciousness often touch on its close relative, self-consciousness. This term, also, has a complex web of senses, probably an even more tangled web than does consciousness itself. At least five senses can be distinguished: (i) proneness to embarrassment: a colloquial sense in which the term refers to excessive sensitivity to the attention of others; (ii) self-detection: a relatively impoverished sense in which the term refers to the ability to detect stimuli directly impinging on the subject (an ant crawling over one’s hand) or actions which the subject has performed; (iii) self-recognition: a sense in which it refers to the more demanding ability to recognize oneself, for example, in a mirror, an ability which apes possess but monkeys do not, and which human children acquire at around the age of 18 months; (iv) awareness of awareness: a sense in which it refers to our ability to interpret our own behavior and that of others in terms of mental states, recognizing ourselves and others not merely as objects— which might be reflected in a mirror—but also as subjects of experience; (v) self-knowledge: a sense in which it refers to our view of ourselves as, for example, members of a particular profession or society, and to our developing understanding, over the course of a lifetime, of ourselves and our reasons for behaving as we do.
THE SCIENCE OF CONSCIOUS STATES
The scientific understanding of wakefulness, sleep, and pathologically altered states of consciousness has been transformed over the 20th century by physiologic, anatomic, and pharmacologic advances.
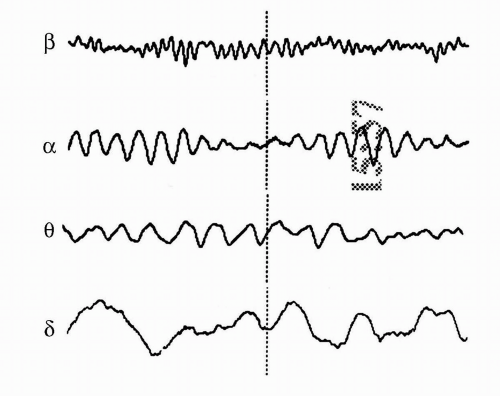
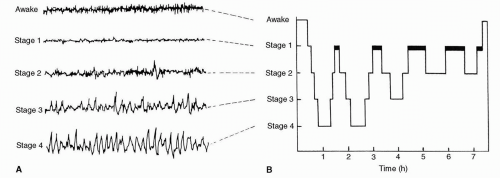
Hans Berger’s demonstration in 1929 illustrated that it was possible to record the brain’s electrical activity from the scalp provided a tool—the EEG—with which to track the concerted shifts in cerebral activity which accompany changes in conscious state (11). Berger and others soon described the fundamental rhythms of the EEG (Fig. 24.1): β, at greater than 14 Hz, which accompanies mental effort; α, at 8-13 Hz, the signature of relaxed wakefulness; θ (4-7 Hz) and δ (less than 4 Hz), which predominate in deep sleep. In the 1950s, Kleitman et al. in Chicago discovered that sleep itself has an internal architecture (12,13). Over the first hour of sleep, the sleeper descends through a series of deepening stages into stage III and IV sleep in which slow waves predominate (slow wave sleep, SWS, known as non-REM, NREM, sleep), only to ascend back through these stages into a state resembling wakefulness in its EEG appearance, accompanied by rapid eye movements, profound muscular atonia, and vivid mentation—dreaming, and paradoxic or rapid eye movement sleep (REM) (Fig. 24.2). This cycle repeats itself four or five times in the course of the night, with decreasing amounts of SWS and increasing amounts of REM as the night proceeds. Recent work on the brain’s electrical rhythms has highlighted the potential importance of rapid, widely synchronized, high frequency γ oscillations (25-100 Hz) in wakefulness and REM (14), although their true significance is not yet clear.
Figure 24.1 The rhythms of the EEG. Records from diagnostic encephalograms performed in four different patients, exemplifying β rhythm (greater than 14 Hz); α rhythm (8-13 Hz); θ rhythm (4-7 Hz); and δ rhythm (<4 Hz). In each case the dotted line bisects a 2-second sample (2).
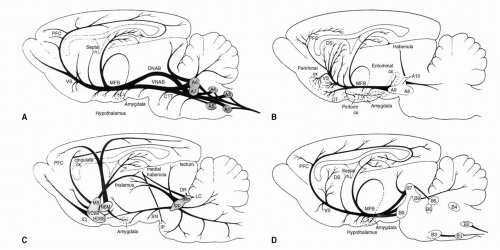
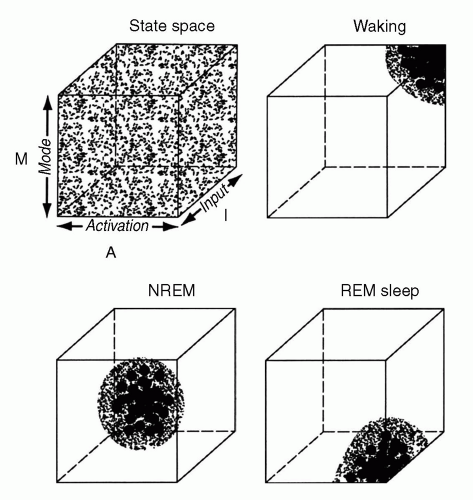
The anatomic and pharmacologic mechanisms which control these cycling states have also been clarified over the past 100 years. Moruzzi and Magoun’s proposal (15) that the brainstem and thalamus are home to an activating system which maintains arousal in the hemispheres has stood the test of time. However, the notion of a monolithic system has given way to a pharmacologically complex picture of multiple interacting activating systems innervating the cerebral hemispheres widely from the brainstem and diencephalon (16) (Fig. 24.3). These systems are defined by their neurotransmitters, which include acetylcholine, serotonin, noradrenaline, dopamine, histamine, hypocretin, and glutamate. The normal succession of conscious states is regulated by these systems (17). For example, in SWS, all these systems become relatively quiescent; in REM periods, the ascending cholinergic system becomes disproportionately active. REM periods are eventually brought to an end by rising levels of activity in noradrenergic and serotonergic neuronal groups which had fallen silent at REM onset. Hobson’s AIM model attempts to integrate several lines of evidence on the genesis and nature of conscious states (Fig. 24.4).
Figure 24.2 The architecture of sleep. An example of sleep staging over the course of a single night. (A) The sleeper passes from wakefulness to deep sleep and then ascends to REM sleep (dark bars). Five similar cycles occur in the course of the night. The EEG tracings (B) show the EEG appearances associated with the stages of sleep; the EEG in REM resembles the “awake” trace. (Kandel ER, Schwartz JH, Jessell TM, eds. Principles of Neural Science. Prentice Hall, 1991.)
Figure 24.3 The pharmacology of the brainstem activating systems. The figure shows (A) the origin and distribution of the central noradrenergic pathways in the rat brain; (B) the dopaminergic pathways; (C) the cholinergic pathways; (D) the serotonergic pathways. CTT, central tegmental tract; dltn, dorsolateral tegmental nucleus; DNAB, dorsal noradrenergic ascending bundle; DR, dorsal raphe; DS, dorsal striatum; HDBB, horizontal limb nucleus of the diagonal band of Broca; Icj, islands of Calleja; IP, interpeduncular nucleus; LC, locus ceruleus; MFB, medial forebrain bundle; MS, medial septum; NBM, nucleus basalis magnocellularis (Meynert in primates); OT, olfactory tubercle; PFC, prefrontal cortex; SN, substantia nigra; tpp, tegmental pedunculopontine nucleus; VDBB, vertical limb nucleus of the diagonal band of Broca; VNAB, ventral noradrenergic ascending bundle; VS, ventral striatum. (Robbins TW, Everitt BJ. Arousal systems and attention. The cognitive neurosciences. Cambridge: MIT Press 1995;703-720.)
Figure 24.4 The AIM model. Hobson’s AIM model locates the three principal states of healthy consciousness in a “state space” defined by input (I: external in wakefulness, internal during REM), activation (A: high in REM and wakefulness, low in NREM sleep), and mode (M: during REM prefrontal regions involved in regulation of waking behaviour and encoding of memories are deactivated). (Hobson JA. Consciousness, sleep and dreaming. In: Nadel L, ed. Macmillan encyclopaedia of cognitive science. Nature Publishing, 2002.)
TABLE 24.1 THE DIFFERENTIAL DIAGNOSIS OF IMPAIRED AWARENESS
Condition
Vegetative State
Minimally Conscious State
Locked-in Syndrome
Coma
Death Confirmed by Brainstem Tests
Awareness
Absent
Present
Present
Absent
Absent
Sleep-wake cycle
Present
Present
Present
Absent
Absent
Response to pain
+/−
Present
Present (in eyes only)
+/−
Absent
Glasgow Coma Score
E4, M1-4, V1-2
E4, M1-5, V1-4
E4, M1, V1
E1,M1-4, V1-2
E1, M1-3, V1
Motor function
No purposeful movement
Some consistent or inconsistent verbal or purposeful motor behavior
Volitional vertical eye movements or eyeblink preserved
Variable: if permanent, continued vegetative state or death
Variable
Depends on cause but full recovery unlikely
Recovery, vegetative state, or death within weeks
Already dead
(Working party of the Royal College of Physicians. The vegetative state: guidance on diagnosis and management. London: Royal College of Physicians of London, 2003.)
Only gold members can continue reading. Log In or Register to continue
 Freud and Psychogenic Movement Disorders
Freud and Psychogenic Movement Disorders
 Functional Paralysis and Sensory Disturbance
Functional Paralysis and Sensory Disturbance
 The Sodium Amytal and Benzodiazepine Interview and Its Possible Application in Psychogenic Movement Disorders
The Sodium Amytal and Benzodiazepine Interview and Its Possible Application in Psychogenic Movement Disorders



