Contributions of the Psychosocial Sciences
 2.1 Jean Piaget and Cognitive Development
2.1 Jean Piaget and Cognitive Development
Jean Piaget (1896–1980) is considered one of the greatest thinkers of the 20th century. His contributions to the understanding of cognitive development had paradigmatic influence in developmental psychology and had major implications for interventions with children, both educational and clinical.
Piaget was born in Neuchatel, Switzerland, where he studied at the university and received a doctorate in biology at the age of 22 (Fig. 2.1-1). Interested in psychology, he studied and carried out research at several centers, including the Sorbonne in Paris, and he worked with Eugen Bleuler at the Burghöltzli Psychiatric Hospital.
FIGURE 2.1-1
Jean Piaget (1896–1980). (Reprinted from the Jean Piaget Society, Temple University, Philadelphia, PA, with permission.)
Piaget created a broad theoretical system for the development of cognitive abilities; in this sense, his work was similar to that of Sigmund Freud, but Piaget emphasized the ways that children think and acquire knowledge.
Widely renowned as a child (or developmental) psychologist, Piaget referred to himself primarily as a genetic epistemologist; he defined genetic epistemology as the study of the development of abstract thought on the basis of a biological or innate substrate. That self-designation reveals that Piaget’s central project was more than the articulation of a developmental child psychology, as this term is generally understood; it was an account of the progressive development of human knowledge.
COGNITIVE DEVELOPMENT STAGES
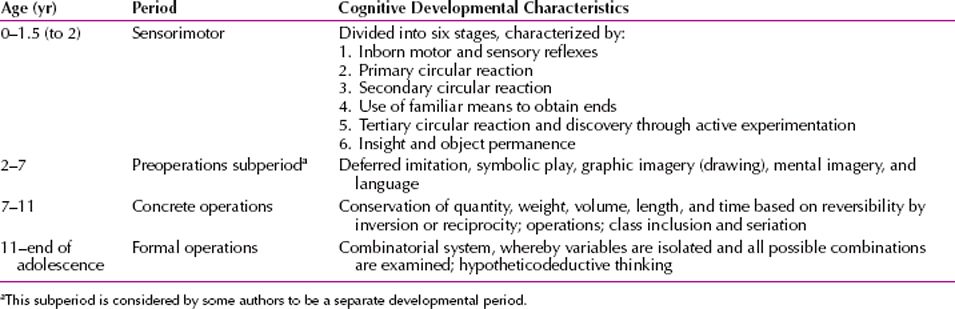
According to Piaget, the following four major stages lead to the capacity for adult thought (Table 2.1-1): (1) sensorimotor, (2) preoperational thought, (3) concrete operations, and (4) formal operations. Each stage is a prerequisite for the following one, but the rate at which different children move through different stages varies with their native endowment and environmental circumstances.
 Table 2.1-1
Table 2.1-1
Stages of Intellectual Development Postulated by Piaget
Sensorimotor Stage (Birth to 2 Years)
Piaget used the term sensorimotor to describe the first stage: Infants begin to learn through sensory observation, and they gain control of their motor functions through activity, exploration, and manipulation of the environment. Piaget divided this stage into six substages, listed in Table 2.1-2.
 Table 2.1-2
Table 2.1-2
Piaget’s Sensorimotor Period of Cognitive Development

From the outset, biology and experience blend to produce learned behavior. For example, infants are born with a sucking reflex, but a type of learning occurs when infants discover the location of the nipple and alter the shape of their mouths. A stimulus is received, and a response results, accompanied by a sense of awareness that is the first schema, or elementary concept. As infants become more mobile, one schema is built on another, and new and more complex schemata are developed. Infants’ spatial, visual, and tactile worlds expand during this period; children interact actively with the environment and use previously learned behavior patterns. For example, having learned to use a rattle, infants shake a new toy as they did the rattle they had already learned to use. Infants also use the rattle in new ways.
The critical achievement of this period is the development of object permanence or the schema of the permanent object. This phrase relates to a child’s ability to understand that objects have an existence independent of the child’s involvement with them. Infants learn to differentiate themselves from the world and are able to maintain a mental image of an object, even when it is not present and visible. When an object is dropped in front of infants, they look down to the ground to search for the object; that is, they behave for the first time as though the object has a reality outside themselves.
At about 18 months, infants begin to develop mental symbols and to use words, a process known as symbolization. Infants are able to create a visual image of a ball or a mental symbol of the word ball to stand for, or signify, the real object. Such mental representations allow children to operate on new conceptual levels. The attainment of object permanence marks the transition from the sensorimotor stage to the preoperational stage of development.
Stage of Preoperational Thought (2 to 7 Years)
During the stage of preoperational thought, children use symbols and language more extensively than in the sensorimotor stage. Thinking and reasoning are intuitive; children learn without the use of reasoning. They are unable to think logically or deductively, and their concepts are primitive; they can name objects but not classes of objects. Preoperational thought is midway between socialized adult thought and the completely autistic Freudian unconscious. Events are not linked by logic. Early in this stage, if children drop a glass that then breaks, they have no sense of cause and effect. They believe that the glass was ready to break, not that they broke the glass. Children in this stage also cannot grasp the sameness of an object in different circumstances: The same doll in a carriage, a crib, or a chair is perceived to be three different objects. During this time, things are represented in terms of their function. For example, a child defines a bike as “to ride” and a hole as “to dig.”
In this stage, children begin to use language and drawings in more elaborate ways. From one-word utterances, two-word phrases develop, made up of either a noun and a verb or a noun and an objective. A child may say, “Bobby eat,” or “Bobby up.”
Children in the preoperational stage cannot deal with moral dilemmas, although they have a sense of what is good and bad. For example, when asked, “Who is more guilty, the person who breaks one dish on purpose or the person who breaks 10 dishes by accident?” a young child usually answers that the person who breaks 10 dishes by accident is more guilty because more dishes are broken. Children in this stage have a sense of immanent justice, the belief that punishment for bad deeds is inevitable.
Children in this developmental stage are egocentric: They see themselves as the center of the universe; they have a limited point of view; and they are unable to take the role of another person. Children are unable to modify their behavior for someone else; for example, children are not being negativistic when they do not listen to a command to be quiet because their brother has to study. Instead, egocentric thinking prevents an understanding of their brother’s point of view.
During this stage, children also use a type of magical thinking, called phenomenalistic causality, in which events that occur together are thought to cause one another (e.g., thunder causes lightning, and bad thoughts cause accidents). In addition, children use animistic thinking, which is the tendency to endow physical events and objects with life-like psychological attributes, such as feelings and intentions.
Semiotic Function. The semiotic function emerges during the preoperational period. With this new ability, children can represent something—such as an object, an event, or a conceptual scheme—with a signifier, which serves a representative function (e.g., language, mental image, symbolic gesture). That is, children use a symbol or sign to stand for something else. Drawing is a semiotic function initially done as a playful exercise but eventually signifying something else in the real world.
Stage of Concrete Operations (7 to 11 Years)
The stage of concrete operations is so named because in this period children operate and act on the concrete, real, and perceivable world of objects and events. Egocentric thought is replaced by operational thought, which involves dealing with a wide array of information outside the child. Therefore, children can now see things from someone else’s perspective.
Children in this stage begin to use limited logical thought processes and can serialize, order, and group things into classes on the basis of common characteristics. Syllogistic reasoning, in which a logical conclusion is formed from two premises, appears during this stage; for example, all horses are mammals (premise); all mammals are warm blooded (premise); therefore, all horses are warm blooded (conclusion). Children are able to reason and to follow rules and regulations. They can regulate themselves, and they begin to develop a moral sense and a code of values.
Children who become overly invested in rules may show obsessive-compulsive behavior; children who resist a code of values often seem willful and reactive. The most desirable developmental outcome in this stage is that a child attains a healthy respect for rules and understands that there are legitimate exceptions to rules.
Conservation is the ability to recognize that, although the shape of objects may change, the objects still maintain or conserve other characteristics that enable them to be recognized as the same. For example, if a ball of clay is rolled into a long, thin sausage shape, children recognize that each form contains the same amount of clay. An inability to conserve (which is characteristic of the preoperational stage) is observed when a child declares that there is more clay in the sausage-shaped piece because it is longer. Reversibility is the capacity to understand the relation between things, to realize that one thing can turn into another and back again—for example, ice and water.
The most important sign that children are still in the preoperational stage is that they have not achieved conservation or reversibility. The ability of children to understand concepts of quantity is one of Piaget’s most important cognitive developmental theories. Measures of quantity include measures of substance, length, number, liquids, and area (Fig. 2.1-2).
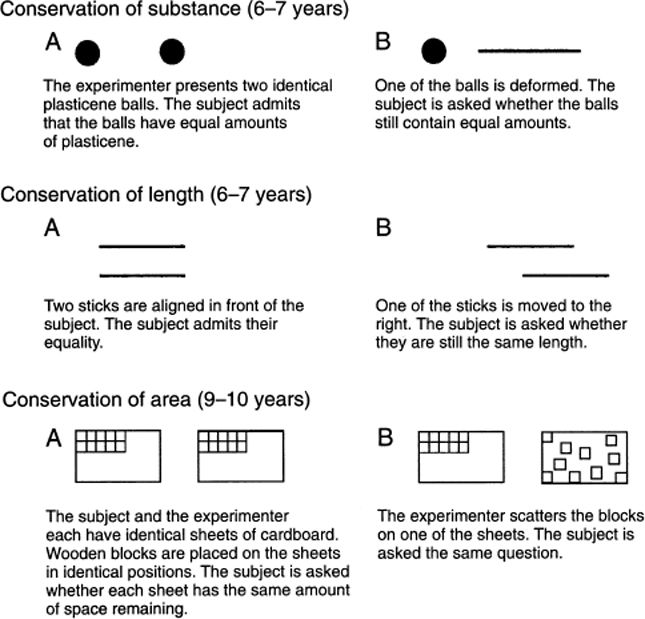
FIGURE 2.1-2
Some simple tests for conservation, with approximate ages of attainment. When the sense of conservation is achieved, the child answers that B contains the same quantity as A. (Modified from Lefrancois GR. Of Children: An Introduction to Child Development. Wadsworth: Belmont, CA; 1973:305, with permission.)
The 7- to 11-year-old child must organize and order occurrences in the real world. Dealing with the future and its possibilities occurs in the formal operational stage.
Stage of Formal Operations (11 through the End of Adolescence)
The stage of formal operations is so named because young persons’ thinking operates in a formal, highly logical, systematic, and symbolic manner. This stage is characterized by the ability to think abstractly, to reason deductively, and to define concepts, and also by the emergence of skills for dealing with permutations and combinations; young persons can grasp the concept of probabilities. Adolescents attempt to deal with all possible relations and hypotheses to explain data and events during this stage. Language use is complex; it follows formal rules of logic and is grammatically correct. Abstract thinking is shown by adolescents’ interest in a variety of issues—philosophy, religion, ethics, and politics.
Hypotheticodeductive Thinking. Hypotheticodeductive thinking, the highest organization of cognition, enables persons to make a hypothesis or proposition and to test it against reality. Deductive reasoning moves from the general to the particular and is a more complicated process than inductive reasoning, which moves from the particular to the general.
Because young persons can reflect on their own and other persons’ thinking, they are susceptible to self-conscious behavior. As adolescents attempt to master new cognitive tasks, they may return to egocentric thought, but on a higher level than in the past. For example, adolescents may think that they can accomplish everything or can change events by thought alone. Not all adolescents enter the stage of formal operations at the same time or to the same degree. Depending on individual capacity and intervening experience, some may not reach the stage of formal operational thought at all and may remain in the concrete operational mode throughout life.
PSYCHIATRIC APPLICATIONS
Piaget’s theories have many psychiatric implications. Hospitalized children who are in the sensorimotor stage have not achieved object permanence and, therefore, have separation anxiety. They do best if their mothers are allowed to stay with them overnight. Children at the preoperational stage, who are unable to deal with concepts and abstractions, benefit more from role-playing proposed medical procedures and situations than by having them verbally described in detail. For example, a child who is to receive intravenous therapy is helped by acting out the procedure with a toy intravenous set and dolls.
Because children at the preoperational stage do not understand cause and effect, they may interpret physical illness as punishment for bad thoughts or deeds; and because they have not yet mastered the capacity to conserve and do not understand the concept of reversibility (which normally occurs during the concrete operational stage), they cannot understand that a broken bone mends or that blood lost in an accident is replaced.
Adolescents’ thinking, during the stage of formal operations, may appear overly abstract when it is, in fact, a normal developmental stage. Adolescent turmoil may not herald a psychotic process but may well result from a normal adolescent’s coming to grips with newly acquired abilities to deal with the unlimited possibilities of the surrounding world.
Adults under stress may regress cognitively as well as emotionally. Their thinking can become preoperational, egocentric, and sometimes animistic.
Implications for Psychotherapy
Piaget was not an applied psychologist and did not develop the implications of his cognitive model for psychotherapeutic intervention. Nevertheless, his work formed one of the foundations of the cognitive revolution in psychology. One aspect of this revolution was an increasing emphasis on the cognitive components of the therapeutic endeavor. In contrast to classical psychodynamic therapy, which focused primarily on drives and affects, and in contrast to behavior therapy, which focused on overt actions, cognitive approaches to therapy focused on thoughts, including automatic assumptions, beliefs, plans, and intentions. By including “theory theory” and “script theory” we can see additional applications to psychotherapy.
Cognitive development theory has influenced psychotherapeutic approaches in multiple ways. Some therapists have taken developmental notions from Piaget’s work and developed intervention techniques. Others have developed cognitive models of treatment independent of Piaget but with heavy reliance on the role of cognition. Others have included Piaget’s concepts in a broader set of constructs to undergird new developmental approaches to psychotherapy.
First, some psychotherapists applied Piagetian notions directly to child interventions. Susan Harter, for example, discussed techniques for helping young children become aware of divergent or contradictory emotions and to integrate these complex emotions within a more abstract or higher class of emotions. One of Harter’s techniques is to ask the young child to make a drawing that shows different and conflicting feelings in one person. This technique represents an application of the concrete operation of class inclusion to the realm of the emotions. Harter’s work applied Piagetian findings to the common therapeutic problem of helping children to recognize, tolerate, and integrate mixed or ambivalent affects within stable object relations.
As such, it drew on cognitive theory and psychodynamic theory. Similar techniques are important in work with children who have been exposed to trauma or to sexual abuse. It is an essential component of such work to assist them in labeling, differentiating, and accepting the full range of emotions stemming from these experiences.
Second, other psychotherapists developed treatment models that, although not directly dependent on Piagetian psychology, emphasized core ideas quite similar to those Piaget discovered in his naturalistic observations of cognitive development. These models are even more closely aligned with recent developments in “theory theory.” Aaron Beck, for example, developed an entire school of cognitive therapy that focuses on the role of cognitions in causing or maintaining psychopathology. Cognitive therapy has been shown to be an effective treatment for problems as diverse as depression, anxiety disorders, and substance abuse.
A core idea in cognitive therapy is that the patient has developed certain core beliefs, aspects of the self-schema, and conditional probability beliefs as a result of developmental experiences, and these contribute to emotional or behavioral problems. For example, depressed persons may have the core belief “I am unlovable.” Addicted persons may have the belief “Unless I drink I cannot feel happy.” In cognitive therapy, the person can be assisted to identify the negative automatic thoughts and underlying dysfunctional attitudes or beliefs that contribute to emotional distress or addictive behavior. The key therapeutic process after identification of the maladaptive thoughts is to help the patient view these thoughts more objectively, not take them in an unquestioning manner as veridical. Here, cognitive therapy emphasizes evidence, consistent both with Piagetian theory and “theory theory.” The patient is assisted to seek out evidence to test negative thinking; active involvement, rather than passive listening, is required.
What the cognitive therapist accomplishes through such techniques as Socratic questioning and asking if there are other ways to look at the same event is similar to what the talented teacher does in guiding children to more adequate, more intelligent understanding of operational tasks. The notion of equilibration is relevant in both instances. By helping the individual see that previous cognitive structures are in some ways inadequate, the therapist or teacher disturbs the old cognitive structure, and the patient or student experiences a disruption that leads to the search for more-adequate structures. The compensation for external disturbance is what Piaget termed equilibration. New structures can be constructed only through a process of accommodation, enabling the subject to assimilate a wider array of data, a new perspective, or more complex information.
Because it requires thinking about thinking, cognitive therapy seems to require formal operational thinking, although this has not been empirically tested. At the least, it requires the ability to recognize and articulate affects, to recognize and label events that give rise to affects, and to translate into a thought the mediating process that occurs rapidly between the event and the affect. Cognitive–behavioral models of psychotherapy include cognitive techniques and more behavioral, interactive techniques, such as increasing pleasant activities and improving communication and problem-solving skills. It is possible that the less-cognitive, more-behavioral techniques, although requiring a lower level of cognitive development, can also lead to garnering of evidence and modification of specific expectancies, attributions, and self-schemata.
Because “script theory” or narrative approaches to cognition in psychotherapy are empirically based, generated by repetitive experiences rather than by reflective abstraction, and domain specific, they may have even more general application to psychotherapy than classic Piagetian theories or “theory theory.” For example, in dialectical behavior therapy, patients provide a “chain analysis” of events, feelings, thoughts, situational stimuli, and interpersonal factors that led up to a negative or self-damaging behavior. This narrative provides guidance to the patient and the therapist about where and how to intervene to prevent subsequent similar behavior.
Developmentally Based Psychotherapy
Developmentally based psychotherapy, developed by Stanley Greenspan, M.D., integrates cognitive, affective, drive, and relationship-based approaches with new understanding of the stages of human development. The clinician first determines the level of the patient’s ego or personality development and the presence or absence of deficits or constrictions. For example, can the person regulate activity and sensations, relate to others, read nonverbal affective symbols, represent experience, build bridges between representations, integrate emotional polarities, abstract feelings, and reflect on internal wishes and feelings?
From a developmental point of view, the integral parts of the therapeutic process include learning how to regulate experience; to engage more fully and deeply in relationships; to perceive, comprehend, and respond to complex behaviors, and interactive patterns; and to be able to engage in the ever-changing opportunities, tasks, and challenges during the course of life (e.g., adulthood and aging) and, throughout, to observe and reflect on one’s own and others’ experiences. These processes are the foundation of the ego, and more broadly, the personality. Their presence constitutes emotional health and their absence, emotional disorder. The developmental approach describes how to harness these core processes and so assist the patients in mobilizing their own growth.
REFERENCES
Bond T. Comparing decalage and development with cognitive developmental tests. J Appl Meas. 2010;11(2):158.
Boom J. Egocentrism in moral development: Gibbs, Piaget, Kohlberg. New Ideas Psychol. 2011;29(3):355.
Dickinson D. Zeroing in on early cognitive development in schizophrenia. Am J Psychiatry. 2014;171:9–12.
Greenspan S, Curry J. Piaget and cognitive development. In: Sadock BJ, Sadock VA, Ruiz P, eds. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry. 9th ed. Vol. 1. Philadelphia: Lippincott Williams & Wilkins; 2009:635.
Harris PL. Piaget on causality: The Whig interpretation of cognitive development. Br J Psychol. 2009;100(S1):229.
Houdé O, Pineau A, Leroux G, Poirel N, Perchey G, Lanoë C, Lubin A, Turbelin MR, Rossi S, Simon G, Delcroix N, Lamberton F, Vigneau M, Wisniewski G, Vicet JR, Mazoyer B. Functional magnetic resonance imaging study of Piaget’s conservation-of-number task in preschool and school-age children: A neo-Piagetian approach. J Exp Child Psychol. 2011;110(3):332
Mesotten D, Gielen M, Sterken C, Claessens K, Hermans G, Vlasselaers D, Lemiere J, Lagae L, Gewillig M, Eyskens B, Vanhorebeek I, Wouters PJ, Van den Berghe G. Neurocognitive development of children 4 years after critical illness and treatment with tight glucose control: A randomized controlled trial. JAMA. 2012;308(16):1641.
Whitbourne SK, Whitbourne SB. Piaget’s cognitive-developmental theory. In: Adult Development and Aging: Biopsychosocial Perspectives. 4th ed. Hoboken: John Wiley & Sons, Inc.; 2011:32.
 2.2 Attachment Theory
2.2 Attachment Theory
ATTACHMENT AND DEVELOPMENT
Attachment can be defined as the emotional tone between children and their caregivers and is evidenced by an infant’s seeking and clinging to the caregiving person, usually the mother. By their first month, infants usually have begun to show such behavior, which is designed to promote proximity to the desired person.
Attachment theory originated in the work of John Bowlby, a British psychoanalyst (1907–1990) (Fig. 2.2-1). In his studies of infant attachment and separation, Bowlby pointed out that attachment constituted a central motivational force and that mother–child attachment was an essential medium of human interaction that had important consequences for later development and personality functioning. Being monotropic, infants tend to attach to one person; but they can form attachments to several persons, such as the father or a surrogate. Attachment develops gradually; it results in an infant’s wanting to be with a preferred person, who is perceived as stronger, wiser, and able to reduce anxiety or distress. Attachment thus gives infants feelings of security. The process is facilitated by interaction between mother and infant; the amount of time together is less important than the amount of activity between the two.
FIGURE 2.2-1
John Bowlby (1907–1990).
The term bonding is sometimes used synonymously with attachment, but the two are different phenomena. Bonding concerns the mother’s feelings for her infant and differs from attachment. Mothers do not normally rely on their infants as a source of security, as is the case in attachment behavior. Much research reveals that the bonding of mother to infant occurs when there is skin-to-skin contact between the two or when other types of contact, such as voice and eye contact, are made. Some workers have concluded that a mother who has skin-to-skin contact with her baby immediately after birth shows a stronger bonding pattern and may provide more attentive care than a mother who does not have this experience. Some researchers have even proposed a critical period immediately after birth, during which such skin-to-skin contact must occur if bonding is to take place. This concept is much disputed: Many mothers are clearly bonded to their infants and display excellent maternal care even though they did not have skin-to-skin contact immediately postpartum. Because human beings can develop representational models of their babies in utero and even before conception, this representational thinking may be as important to the bonding process as skin, voice, or eye contact.
Ethological Studies
Bowlby suggested a Darwinian evolutionary basis for attachment behavior; namely, such behavior ensures that adults protect their young. Ethological studies show that nonhuman primates and other animals exhibit attachment behavior patterns that are presumably instinctual and are governed by inborn tendencies. An example of an instinctual attachment system is imprinting, in which certain stimuli can elicit innate behavior patterns during the first few hours of an animal’s behavioral development; thus, the animal offspring becomes attached to its mother at a critical period early in its development. A similar sensitive or critical period during which attachment occurs has been postulated for human infants. The presence of imprinting behavior in humans is highly controversial, but bonding and attachment behavior during the first year of life closely approximate the critical period; in humans, however, this period occurs over a span of years rather than hours.
Harry Harlow. Harry Harlow’s work with monkeys is relevant to attachment theory. Harlow demonstrated the emotional and behavioral effects of isolating monkeys from birth and keeping them from forming attachments. The isolates were withdrawn, unable to relate to peers, unable to mate, and incapable of caring for their offspring.
PHASES OF ATTACHMENT
In the first attachment phase, sometimes called the preattachment stage (birth to 8 or 12 weeks), babies orient to their mothers, follow them with their eyes over a 180-degree range, and turn toward and move rhythmically with their mother’s voice. In the second phase, sometimes called attachment in the making (8 to 12 weeks to 6 months), infants become attached to one or more persons in the environment. In the third phase, sometimes called clear-cut attachment (6 through 24 months), infants cry and show other signs of distress when separated from the caretaker or mother; this phase can occur as early as 3 months in some infants. On being returned to the mother, the infant stops crying and clings, as if to gain further assurance of the mother’s return. Sometimes, seeing the mother after a separation is sufficient for crying to stop. In the fourth phase (25 months and beyond), the mother figure is seen as independent, and a more complex relationship between the mother and the child develops. Table 2.2-1 summarizes the development of normal attachment from birth through 3 years.
 Table 2.2-1
Table 2.2-1
Normal Attachment
Mary Ainsworth
Mary Ainsworth (1913–1999) was a Canadian developmental psychologist from the University of Toronto. She described three main types of insecure attachment: insecure–avoidant, insecure–ambivalent, and insecure–disorganized. The insecure–avoidant child, having experienced brusque or aggressive parenting, tends to avoid close contact with people and lingers near caregivers rather than approaching them directly when faced with a threat. The insecure–ambivalent child finds exploratory play difficult, even in the absence of danger, and clings to his or her inconsistent parents. Insecure–disorganized children have parents who are emotionally absent with a parental history of abuse in their childhood. These children tend to behave in bizarre ways when threatened. According to Ainsworth, disorganization is a severe form of insecure attachment and a possible precursor of severe personality disorder and dissociative phenomena in adolescence and early adulthood.
Mary Ainsworth expanded on Bowlby’s observations and found that the interaction between the mother and her baby during the attachment period significantly influences the baby’s current and future behavior. Patterns of attachments vary among babies; for example, some babies signal or cry less than others. Sensitive responsiveness to infant signals, such as cuddling a crying baby, causes infants to cry less in later months, rather than reinforcing crying behavior. Close bodily contact with the mother when the baby signals for her is also associated with the growth of self-reliance, rather than a clinging dependence, as the baby grows older. Unresponsive mothers produce anxious babies; these mothers often have lower intelligence quotients (IQs) and are emotionally more immature and younger than responsive mothers.
Ainsworth also confirmed that attachment serves to reduce anxiety. What she called the secure base effect enables children to move away from attachment figures and to explore the environment. Inanimate objects, such as a teddy bear and a blanket (called the transitional object by Donald Winnicott), also serve as a secure base, one that often accompanies them as they investigate the world.
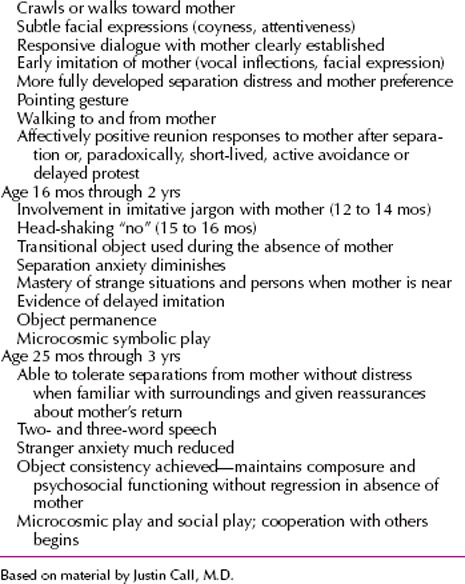
Strange Situation. Ainsworth developed strange situation, the research protocol for assessing the quality and security of an infant’s attachment. In this procedure, the infant is exposed to escalating amounts of stress; for example, the infant and the parent enter an unfamiliar room, an unfamiliar adult then enters the room, and the parent leaves the room. The protocol has seven steps (Table 2.2-2). According to Ainsworth’s studies, about 65 percent of infants are securely attached by the age of 24 months.
 Table 2.2-2
Table 2.2-2
The Strange Situation
ANXIETY
Bowlby’s theory of anxiety holds that a child’s sense of distress during separation is perceived and experienced as anxiety and is the prototype of anxiety. Any stimuli that alarm children and cause fear (e.g., loud noises, falling, and cold blasts of air) mobilize signal indicators (e.g., crying) that cause the mother to respond in a caring way by cuddling and reassuring the child. The mother’s ability to relieve the infant’s anxiety or fear is fundamental to the growth of attachment in the infant. When the mother is close to the child and the child experiences no fear, the child gains a sense of security, the opposite of anxiety. When the mother is unavailable to the infant because of physical absence (e.g., if the mother is in prison) or because of psychological impairment (e.g., severe depression), anxiety develops in the infant.
Expressed as tearfulness or irritability, separation anxiety is the response of a child who is isolated or separated from its mother or caretaker. It is most common at 10 to 18 months of age and disappears generally by the end of the third year. Somewhat earlier (at about 8 months) stranger anxiety, an anxiety response to someone other than the caregiver, appears.
Signal Indicators
Signal indicators are infants’ signs of distress that prompt or elicit a behavioral response in the mother. The primary signal is crying. The three types of signal indicators are hunger (the most common), anger, and pain. Some mothers can distinguish between them, but most mothers generalize the hunger cry to represent distress from pain, frustration, or anger. Other signal indicators that reinforce attachment are smiling, cooing, and looking. The sound of an adult human voice can prompt these indicators.
Losing Attachments
Persons’ reactions to the death of a parent or a spouse can be traced to the nature of their past and present attachment to the lost figure. An absence of demonstrable grief may be owing to real experiences of rejection and to the lack of closeness in the relationship. The person may even consciously offer an idealized picture of the deceased. Persons who show no grief usually try to present themselves as independent and as disinterested in closeness and attachment.
Sometimes, however, the severing of attachments is traumatic. The death of a parent or a spouse can precipitate a depressive disorder, and even suicide, in some persons. The death of a spouse increases the chance that the surviving spouse will experience a physical or mental disorder during the next year. The onset of depression and other dysphoric states often involves having been rejected by a significant figure in a person’s life.
DISORDERS OF ATTACHMENT
Attachment disorders are characterized by biopsychosocial pathology that results from maternal deprivation, a lack of care by, and interaction with, the mother or caregiver. Failure-to-thrive syndromes, psychosocial dwarfism, separation anxiety disorder, avoidant personality disorder, depressive disorders, delinquency, academic problems, and borderline intelligence have been traced to negative attachment experiences. When maternal care is deficient because (1) a mother is mentally ill, (2) a child is institutionalized for a long time, or (3) the primary object of attachment dies, children sustain emotional damage. Bowlby originally thought that the damage was permanent and invariable, but he revised his theories to take into account the time at which the separation occurred, the type and degree of separation, and the level of security that the child experienced before the separation.
Bowlby described a predictable set and sequence of behavior patterns in children who are separated from their mothers for long periods (more than 3 months): protest, in which the child protests the separation by crying, calling out, and searching for the lost person; despair, in which the child appears to lose hope that the mother will return; and detachment, in which the child emotionally separates himself or herself from the mother. Bowlby believed that this sequence involves ambivalent feelings toward the mother; the child both wants her and is angry with her for her desertion.
Children in the detachment stage respond in an indifferent manner when the mother returns; the mother has not been forgotten, but the child is angry at her for having gone away in the first place and fears that she will go away again. Some children have affectionless personalities characterized by emotional withdrawal, little or no feeling, and a limited ability to form affectionate relationships.
Anaclitic Depression
Anaclitic depression, also known as hospitalism, was first described by René Spitz in infants who had made normal attachments but were then suddenly separated from their mothers for varying times and placed in institutions or hospitals. The children became depressed, withdrawn, nonresponsive, and vulnerable to physical illness, but they recovered when their mothers returned or when surrogate mothering was available.
CHILD MALTREATMENT
Abused children often maintain their attachments to abusive parents. Studies of dogs have shown that severe punishment and maltreatment increase attachment behavior. When children are hungry, sick, or in pain, they too show clinging attachment behavior. Similarly, when children are rejected by their parents or are afraid of them, their attachment may increase; some children want to remain with an abusive parent. Nevertheless, when a choice must be made between a punishing and a nonpunishing figure, the nonpunishing person is the preferable choice, especially if the person is sensitive to the child’s needs.
PSYCHIATRIC APPLICATIONS
The applications of attachment theory in psychotherapy are numerous. When a patient is able to attach to a therapist, a secure base effect is seen. The patient may then be able to take risks, mask anxiety, and practice new patterns of behavior that otherwise might not have been attempted. Patients whose impairments can be traced to never having made an attachment in early life may do so for the first time in therapy, with salutary effects.
Patients whose pathology stems from exaggerated early attachments may attempt to replicate them in therapy. Therapists must enable such patients to recognize the ways their early experiences have interfered with their ability to achieve independence.
For patients who are children and whose attachment difficulties may be more apparent than those of adults, therapists represent consistent and trusted figures who can engender a sense of warmth and self-esteem in children, often for the first time.
Relationship Disorders
A person’s psychological health and sense of well-being depend significantly on the quality of his or her relationships and attachment to others, and a core issue in all close personal relationships is establishing and regulating that connection. In a typical attachment interaction, one person seeks more proximity and affection, and the other either reciprocates, rejects, or disqualifies the request. A pattern is shaped through repeated exchanges. Distinct attachment styles have been observed. Adults with an anxious–ambivalent attachment style tend to be obsessed with romantic partners, suffer from extreme jealousy, and have a high divorce rate. Persons with an avoidant attachment style are relatively uninvested in close relationships, although they often feel lonely. They seem afraid of intimacy and tend to withdraw when there is stress or conflict in the relationship. Break-up rates are high. Persons with a secure attachment style are highly invested in relationships and tend to behave without much possessiveness or fear of rejection.
REFERENCES
Freud S. The Standard Edition of the Complete Psychological Works of Sigmund Freud. 24 vols. London: Hogarth Press; 1953–1974
Greenberg JR, Mitchell SA. Object Relations in Psychoanalytic Theory. Cambridge, MA: Harvard University Press; 1983.
Laplanche J, Pontalis J-B. The Language of Psycho-analysis. New York: Norton; 1973.
Mahler MS, Pine F, Bergman A. The Psychological Birth of the Human Infant. New York: Basic Books; 1975.
Pallini S, Baiocco R, Schneider BH, Madigan S, Atkinson L. Early child–parent attachment and peer relations: A meta-analysis of recent research. J Fam Psychol. 2014;28:118.
Stern D. The Interpersonal World of the Infant. New York: Basic Books; 1985.
Meissner, W.W. Theories of Personality in Psychotherapy. In: Sadock BJ, Sadock VA, eds. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry. 9th ed. Vol. 1. Philadelphia: Lippincott Williams & Wilkins; 2009:788.
 2.3 Learning Theory
2.3 Learning Theory
Learning is defined as a change in behavior resulting from repeated practice. The principles of learning are always operating and always influencing human activity. Learning principles are often deeply involved in the etiology and maintenance of psychiatric disorders because so much of human behavior (including overt behavior, thought patterns, and emotion) is acquired through learning. Learning processes also strongly influence psychotherapy because human behavior changes. Thus, learning principles can influence the effectiveness of therapy. In fact, no method of therapy can be said to be immune to the effects of learning. Even the simple prescription of a medication can bring learning processes into play because the patient will have opportunities to learn about the drug’s effects and side effects, will need to learn to comply with the instructions and directions for taking it, and will need to learn to overcome any resistance to compliance.
BASIC CONCEPTS AND CONSIDERATIONS
A great deal of modern research on learning still focuses on Pavlovian (classical) and operant learning. Pavlovian conditioning, developed by Ivan Petrovich Pavlov (1849–1936), occurs when neutral stimuli are associated with a psychologically significant event. The main result is that the stimuli come to evoke a set of responses or emotions that may contribute to many clinical disorders, including (but not limited to) anxiety disorders and drug dependence. The events in Pavlov’s experiment are often described using terms designed to make the experiment applicable to any situation. The food is the unconditional stimulus (US) because it unconditionally elicits salivation before the experiment begins. The bell is known as the conditional stimulus (CS) because it only elicits the salivary response conditional on the bell–food pairings. The new response to the bell is correspondingly called the conditional response (CR), and the natural response to the food itself is the unconditional response (UR). Modern laboratory studies of conditioning use a very wide range of CSs and USs and measure a wide range of conditioned responses.
Operant conditioning, developed by B.F. Skinner (1904–1990), occurs when a behavior (instead of a stimulus) is associated with a psychologically significant event. In the laboratory, the most famous experimental arrangement is the one in which a rat presses a lever to earn food pellets. In this case, as opposed to Pavlov’s, the behavior is said to be an operant because it operates on the environment. The food pellet is a reinforcer—an event that increases the strength of the behavior of which it is made a consequence. A major idea behind this method is that the rat’s behavior is “voluntary” in the sense that the animal is not compelled to make the response (it can perform it whenever it “wants” to). In this sense, it is similar to the thousands of operant behaviors that humans choose to commit—freely—in any day. Of course, the even larger idea is that even though the rat’s behavior appears as though it is voluntary, it is lawfully controlled by its consequences: If the experimenter were to stop delivering the food pellet, the rat would stop pressing the lever, and if the experimenter were to allow the lever press to produce larger pellets, or perhaps pellets at a higher probability or rate, then the rate of the behavior might increase. The point of operant conditioning experiments, then, is largely to understand the relation of behavior to its payoff.
Pavlovian and operant conditioning differ in several ways. One of the most fundamental differences is that the responses observed in Pavlov’s experiment are elicited and thus controlled by the presentation of an antecedent stimulus. In contrast, the “response” observed in Skinner’s experiment is not elicited or compelled by an antecedent stimulus in any obvious way—it is instead controlled by its consequences. This distinction between operants and respondents is important in clinical settings. If a young patient is referred to the clinic for acting out in the classroom, an initial goal of the clinician will be to determine whether the behavior is a respondent or an operant, and then the clinician will go about changing either its antecedents or its consequences, respectively, to reduce its probability of occurrence.
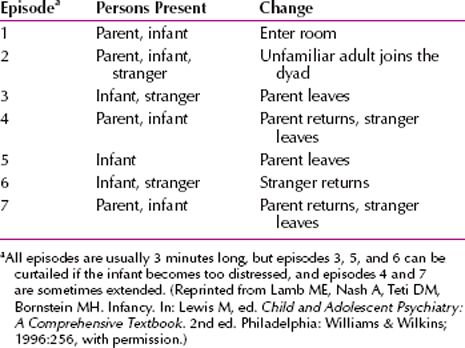
Despite the academic separation of operant and respondent conditioning, they have an important common function: Both learning processes are designed by evolution to allow organisms to adapt to the environment. The idea is illustrated by considering the law of effect (Fig. 2.3-1), which says that whether an operant behavior increases or decreases in strength depends on the effect it has on the environment. When the action leads to a positive outcome, the action is strengthened; conversely, when the action leads to a negative outcome, we have punishment, and the action is weakened. In a similar manner, when an action decreases the probability of a positive event, behavior also declines. (Such a procedure is now widely known as time-out from reinforcement.) When an action terminates or prevents the occurrence of a negative event, the behavior will strengthen. By thus enabling the organism to maximize its interaction with positive events and minimize its interaction with negative ones, operant conditioning allows the organism to optimize its interaction with the environment. Of course, events that were once positive in the human’s earlier evolutionary history are so prevalent in modern society that they do not always seem adaptive today. Thus, reward learning also provides a framework for understanding the development of rather maladaptive behaviors like overeating (in which behavior is reinforced by food) and drug taking (in which behaviors are reinforced by the pharmacological effects of drugs)—cases in which reward principles lead to psychopathology.
FIGURE 2.3-1
The law of effect in instrumental/operant learning. Actions either produce or prevent good or bad events, and the strength of the action changes accordingly (arrow). “Reinforcement” refers to a strengthening of behavior. Positive reinforcement occurs when an action produces a positive event, whereas negative reinforcement occurs when an action prevents or eliminates a negative event. (Courtesy of Mark E. Bouton, PhD.)
A parallel to Figure 2.3-1 exists in Pavlovian conditioning, in which one can likewise think of whether the CS is associated with positive or negative events (Fig. 2.3-2). Although such learning can lead to a wide constellation or system of behaviors, in a very general way, it also leads to behavioral tendencies of approach or withdrawal. Thus, when a CS signals a positive US, the CS will tend to evoke approach behaviors—called sign tracking. For example, an organism will approach a signal for food. Analogously, when a CS signals a negative US, it will evoke behaviors that tend to move the organism away from the CS. Conversely, CSs associated with a decrease in the probability of a good thing will elicit withdrawal behaviors, whereas CSs associated with the decrease in the probability of a bad thing can elicit approach. An example of the latter case might be a stimulus that signals safety or the decrease in probability of an aversive event, which evokes approach in a frightened organism. In the end, these very basic behavioral effects of both operant (see Fig. 2.3-1) and Pavlovian (see Fig. 2.3-2) learning serve to maximize the organism’s contact with good things and minimize contact with bad things.
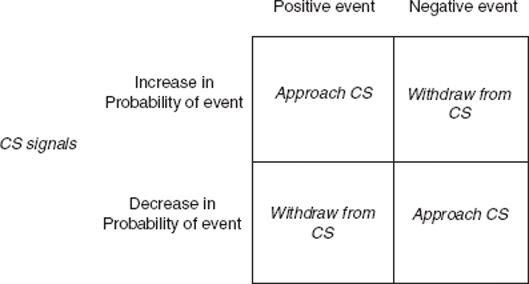
FIGURE 2.3-2
Sign tracking in Pavlovian learning. Conditional stimuli (CSs) signal either an increase or a decrease in the probability of good or bad events, and the CS generally engages approach or withdrawal behaviors accordingly. (Courtesy of Mark E. Bouton, PhD.)
Perhaps because they have such similar functions, Pavlovian learning and operant learning are both influenced by similar variables. For example, in either case, behavior is especially strong if the magnitude of the US or reinforcer is large, or if the US or reinforcer occurs relatively close to the CS or operant response in time. In either case, the learned behavior decreases if the US or reinforcer that was once paired with the CS or the response is eliminated from the situation. This phenomenon, called extinction, provides a means of eliminating unwanted behaviors that were learned through either form of conditioning and has led to a number of very effective cognitive–behavioral therapies.
PAVLOVIAN CONDITIONING
Effects of Conditioning on Behavior
Many lay people have the mistaken impression that Pavlovian learning is a rigid affair in which a fixed stimulus comes to elicit a fixed response. In fact, conditioning is considerably more complex and dynamic than that. For example, signals for food may evoke a large set of responses that function to prepare the organism to digest food: They can elicit the secretion of gastric acid, pancreatic enzymes, and insulin in addition to Pavlov’s famous salivary response. The CS can also elicit approach behavior (as described earlier), an increase in body temperature, and a state of arousal and excitement. When a signal for food is presented to a satiated animal or human, he or she may eat more food. Some of these effects may be motivational; for example, an additional effect of presenting a CS for food is that it can invigorate ongoing operant behaviors that have been reinforced with food. CSs thus have powerful behavioral potential. Signals for food evoke a whole behavior system that is functionally organized to find, procure, and consume food.
Pavlovian conditioning is also involved in other aspects of eating. Through conditioning, humans and other animals may learn to like or dislike certain foods. In animals like rats, flavors associated with nutrients (sugars, starches, calories, proteins, or fats) come to be preferred. Flavors associated with sweet tastes are also preferred, whereas flavors associated with bitter tastes are avoided. At least as important, flavors associated with illness become disliked, as illustrated by the person who gets sick drinking an alcoholic beverage and consequently learns to hate the flavor. The fact that flavor CSs can be associated with such a range of biological consequences (USs) is important for omnivorous animals that need to learn about new foods. It also has some clinical implications. For example, chemotherapy can make cancer patients sick, and it can therefore cause the conditioning of an aversion to a food that was eaten recently (or to the clinic itself). Other evidence suggests that animals may learn to dislike food that is associated with becoming sick with cancer. On the flip side, conditioning can enable external cues to trigger food consumption and craving, a potential influence on overeating and obesity.
Pavlovian conditioning also occurs when organisms ingest drugs. Whenever a drug is taken, in addition to reinforcing the behaviors that lead to its ingestion, the drug constitutes a US and may be associated with potential CSs that are present at the time (e.g., rooms, odors, injection paraphernalia,). CSs that are associated with drug USs can sometimes have an interesting property: They often elicit a conditioned response that seems opposite to the unconditional effect of the drug. For example, although morphine causes a rat to feel less pain, a CS associated with morphine elicits an opposite increase, not a decrease in pain sensitivity. Similarly, although alcohol can cause a drop in body temperature, a conditioned response to a CS associated with alcohol is typically an increase in body temperature. In these cases, the conditioned response is said to be compensatory because it counteracts the drug effect. Compensatory responses are another example of how classical (Pavlovian) conditioning helps organisms prepare for a biologically significant US.
Compensatory conditioned responses have implications for drug abuse. First, they can cause drug tolerance, in which repeated administration of a drug reduces its effectiveness. As a drug and a CS are repeatedly paired, the compensatory response to the CS becomes stronger and more effective at counteracting the effect of the drug. The drug therefore has less impact. One implication is that tolerance will be lost if the drug is taken without being signaled by the usual CS. Consistent with this idea, administering a drug in a new environment can cause a loss of drug tolerance and make drug overdose more likely. A second implication stems from the fact that compensatory responses may be unpleasant or aversive. A CS associated with an opiate may elicit several compensatory responses—it may cause the drug user to be more sensitive to pain, undergo a change in body temperature, and perhaps become hyperactive (the opposite of another unconditional opiate effect). The unpleasantness of these responses may motivate the user to take the drug again to get rid of them, an example of escape learning, or negative reinforcement, and a classic example of how Pavlovian and operant learning processes might readily interact. The idea is that the urge to take drugs may be strongest in the presence of CSs that have been associated with the drug. The hypothesis is consistent with self-reports of abusers, who, after a period of abstinence, are tempted to take the drug again when they are reexposed to drug-associated cues.
Pavlovian learning may potentially be involved in anxiety disorders. CSs associated with frightening USs can elicit a whole system of conditioned fear responses, broadly designed to help the organism cope. In animals, cues associated with frightening events (such as a brief foot shock) elicit changes in respiration, heart rate, and blood pressure, and even a (compensatory) decrease in sensitivity to pain. Brief CSs that occur close to the US in time can also elicit adaptively timed protective reflexes. For example, the rabbit blinks in response to a brief signal that predicts a mild electric shock near the eye. The same CS, when lengthened in duration and paired with the same US, elicits mainly fear responses, and fear elicited by a CS may potentiate the conditioned eyeblink response elicited by another CS or a startle response to a sudden noise. Once again, CSs do not merely elicit a simple reflex, but also evoke a complex and interactive set of responses.
Classical fear conditioning can contribute to phobias (in which specific objects may be associated with a traumatic US), as well as other anxiety disorders, such as panic disorder and posttraumatic stress disorder (PTSD). In panic disorder, people who have unexpected panic attacks can become anxious about having another one. In this case, the panic attack (the US or UR) may condition anxiety to the external situation in which it occurs (e.g., a crowded bus) and also internal (“interoceptive”) CSs created by early symptoms of the attack (e.g., dizziness or a sudden pounding of the heart). These CSs may then evoke anxiety or panic responses. Panic disorder may begin because external cues associated with panic can arouse anxiety, which may then exacerbate the next unconditional panic attack and/or panic response elicited by an interoceptive CS. It is possible that the emotional reactions elicited by CSs may not require conscious awareness for their occurrence or development. Indeed, fear conditioning may be independent of conscious awareness.
In addition to eliciting conditioned responses, CSs also motivate ongoing operant behavior. For example, presenting a CS that elicits anxiety can increase the vigor of operant behaviors that have been learned to avoid or escape the frightening US. Thus, an individual with an anxiety disorder will be more likely to express avoidance in the presence of anxiety or fear cues. Similar effects may occur with CSs that predict other USs (such as drugs or food)—as already mentioned, a drug-associated CS may motivate the drug abuser to take more drugs. The motivating effects of CSs may stem from the fact that CSs may be associated with both the sensory and emotional properties of USs. For example, the survivor of a traumatic train derailment might associate stimuli that occur immediately before derailment (such as the blue flash that occurs when the train separates from its overhead power supply) with both the emotional and the sensory aspects of the crash. Consequently, when the survivor later encounters another flashing blue light (e.g., the lights on a police car), the CS might evoke both emotional responses (mediated by association with the trauma’s emotional qualities) and sensory associations (mediated by association with the trauma’s sensory qualities). Both might play a role in the nightmares and “re-experiencing” phenomena that are characteristic of PTSD.
The Nature of the Learning Process
Research beginning in the late 1960s began to uncover some important details about the learning process behind Pavlovian conditioning. Several findings proved especially important. It was shown, for example, that conditioning is not an inevitable consequence of pairing a CS with a US. Such pairings will not cause conditioning if there is a second CS present that already predicts the US. This finding (known as blocking) suggests that a CS must provide new information about the US if learning is to occur. The importance of the CS’s information value is also suggested by the fact that a CS will not be treated as a signal for the US if the US occurs equally often (or is equally probable) in the presence and the absence of the CS. Instead, the organism treats the CS as a signal for the US if the probability of the US is greater in the presence of the CS than in its absence. In addition, the organism will treat the CS as a signal for “no US” if the probability of the US is less in the presence of the CS than in its absence. In the latter case, the signal is called a conditioned inhibitor because it will inhibit performance elicited by other CSs. The conditioned inhibition phenomenon is clinically relevant because inhibitory CSs may hold pathological CRs like fear or anxiety at bay. A loss of the inhibition would allow the anxiety response to emerge.
There are also important variants of classical conditioning. In sensory preconditioning, two stimuli (A and B) are first paired, and then one of them (A) is later paired with the US. Stimulus A evokes conditioned responding, of course, but so does stimulus B—indirectly, through its association with A. One implication is that exposure to a potent US like a panic attack may influence reactions to stimuli that have never been paired with the US directly; the sudden anxiety to stimulus B might seem spontaneous and mysterious. A related finding is second-order conditioning. Here, A is paired with a US first and then subsequently paired with stimulus B. Once again, both A and B will evoke responding. Sensory preconditioning and second-order conditioning increase the range of stimuli that can control the conditioned response. A third variant worth mentioning occurs, as indicated previously, when the onset of a stimulus becomes associated with the rest of that stimulus, as when a sudden increase in heart rate caused by the onset of a panic attack comes to predict the rest of the panic or feeling, or when the onset of a drug may predict the rest of the drug effect. Such intraevent associations may play a role in many of the body’s regulatory functions, such that an initial change in some variable (e.g., blood pressure or blood glucose level) may come to signal a further increase in that variable and therefore initiate a conditioned compensatory response.
Emotional responses can also be conditioned through observation. For example, a monkey that merely observes another monkey being frightened by a snake can learn to be afraid of the snake. The observer learns to associate the snake (CS) with its emotional reaction (US/UR) to the other monkey being afraid. Although monkeys readily learn to fear snakes, they are less likely to associate other salient cues (such as colorful flowers) with fear in the same way. This is an example of preparedness in classical conditioning—some stimuli are especially effective signals for some USs because evolution has made them that way. Another example is the fact that tastes are easily associated with illness but not shock, whereas auditory and visual cues are easily associated with shock but not illness. Preparedness may explain why human phobias tend to be for certain objects (snakes or spiders) and not others (knives or electric sockets) that may as often be paired with pain or trauma.
Erasing Pavlovian Learning
If Pavlovian learning plays a role in the etiology of behavioral and emotional disorders, a natural question concerns how to eliminate it or undo it. Pavlov studied extinction: Conditioned responding decreases if the CS is presented repeatedly without the US after conditioning. Extinction is the basis of many behavioral or cognitive–behavioral therapies designed to reduce pathological conditioned responding through repeated exposure to the CS (exposure therapy), and it is presumably a consequence of any form of therapy in the course of which the patient learns that previous harmful cues are no longer harmful. Another elimination procedure is counterconditioning, in which the CS is paired with a very different US/UR. Counterconditioning was the inspiration for systematic desensitization, a behavior therapy technique in which frightening CSs are deliberately associated with relaxation during therapy.
Although extinction and counterconditioning reduce unwanted conditioned responses, they do not destroy the original learning, which remains in the brain, ready to return to behavior under the right circumstances. For example, conditioned responses that have been eliminated by extinction or counterconditioning can recover if time passes before the CS is presented again (spontaneous recovery). Conditioned responses can also return if the patient returns to the context of conditioning after extinction in another context, or if the CS is encountered in a context that differs from the one in which extinction has occurred (all are examples of the renewal effect). The renewal effect is important because it illustrates the principle that extinction performance depends on the organism being in the context in which extinction was learned. If the CS is encountered in a different context, the extinguished behavior may relapse or return. Recovery and relapse can also occur if the current context is associated again with the US (“reinstatement”) or if the CS is paired with the US again (“rapid reacquisition”). One theoretical approach assumes that extinction and counterconditioning do not destroy the original learning but instead entail new learning that gives the CS a second meaning (e.g., “the CS is safe” in addition to “the CS is dangerous”). As with an ambiguous word, which has more than one meaning, responding evoked by an extinguished or counterconditioned CS depends fundamentally on the current context.
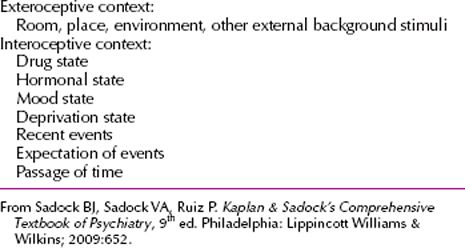
Research on context effects in both animal and human learning and memory suggests that a wide variety of stimuli can play the role of context (Table 2.3-1). Drugs, for example, can be very salient in this regard. When rats are given fear extinction while under the influence of a benzodiazepine tranquilizer or alcohol, fear is renewed when the CS is tested in the absence of the context provided by the drug. This is an example of state-dependent learning, in which the retention of information is best when tested in the same state in which it was originally learned. State-dependent fear extinction has obvious implications for combining therapy with drugs. It also has implications for the administration of drugs more generally. For example, if a person were to take a drug to reduce anxiety, the anxiety reduction would reinforce drug taking. State-dependent extinction might further preserve any anxiety that might otherwise be extinguished during natural exposure to the anxiety-eliciting cues. Thus, drug use could paradoxically preserve the original anxiety, creating a self-perpetuating cycle that could provide a possible explanation for the link between anxiety disorders and substance abuse. One point of this discussion is that drugs can play multiple roles in learning: They can be USs or reinforcers on one hand, and CSs or contexts on the other. The possible complex behavioral effects of drugs are worth bearing in mind.
 Table 2.3-1
Table 2.3-1
Effective Contextual Stimuli Studied In Animal and Human Research Laboratories
Another general message is that contemporary theory emphasizes the fact that extinction (and other processes, such as counterconditioning) entails new learning rather than a destruction of the old. Recent psychopharmacological research has built on this idea: If extinction and therapy constitute new learning, then drugs that might facilitate new learning might also facilitate the therapy process. For example, there has been considerable recent interest in D-cycloserine, a partial agonist of the N-methyl-D-aspartate (NMDA) glutamate receptor. The NMDA receptor is involved in long-term potentiation, a synaptic facilitation phenomenon that has been implicated in several examples of learning. Of interest, there is evidence that the administration of D-cycloserine can facilitate extinction learning in rats and possibly in humans undergoing exposure therapy for anxiety disorders. In the studies supporting this conclusion, the administration of the drug increased the amount of extinction that was apparent after a small (and incomplete) number of extinction trials. Although such findings are promising, it is important to remember that the context dependence of extinction, and thus the possibility of relapse with a change of context, may easily remain. Consistent with this possibility, although D-cycloserine allows fear extinction to be learned in fewer trials, it does not appear to prevent or reduce the strength of the renewal effect. Such results further underscore the importance of behavioral research—and behavioral theory—in understanding the effects of drugs on therapy. Nonetheless, the search for drugs that might enhance the learning that occurs in therapy situations will continue to be an important area of research.
Another process that might theoretically modify or erase a memory is illustrated by a phenomenon called reconsolidation. Newly learned memories are temporarily labile and easy to disrupt before they are consolidated into a more stable form in the brain. The consolidation of memory requires the synthesis of new proteins and can be blocked by the administration of protein synthesis inhibitors (e.g., anisomycin). Animal research suggests that consolidated memories that have recently been reactivated might also return briefly to a similarly vulnerable state; their “reconsolidation” can likewise be blocked by protein synthesis inhibitors. For example, several studies have shown that the reactivation of a conditioned fear by one or two presentations of the CS after a brief fear conditioning experience can allow it to be disrupted by anisomycin. When the CS is tested later, there is little evidence of fear—as if reactivation and then drug administration diminished the strength of the original memory. However, like the effects of extinction, these fear-diminishing effects do not necessarily mean that the original learning has been destroyed or erased. There is some evidence that fear of the CS that has been diminished in this way can still return over time (i.e., spontaneously recover) or with reminder treatments. This sort of result suggests that the effect of the drug is somehow able to interfere with retrieval or access to the memory rather than to be an actual “reconsolidation.”
Generally speaking, the elimination of a behavior after therapy should not be interpreted as erasure of the underlying knowledge. For the time being, it may be safest to assume that after any therapeutic treatment, a part of the original learning may remain in the brain, ready to produce relapse if retrieved. Instead of trying to find treatments that destroy the original memory, another therapeutic strategy might be to accept the possible retention of the original learning and build therapies that allow the organism to prevent or cope with its retrieval. One possibility is to conduct extinction exposure in the contexts in which relapse might be most problematic to the patient and to encourage retrieval strategies (such as the use of retrieval cues like reminder cards) that might help to remind the patient of the therapy experience.
OPERANT/INSTRUMENTAL LEARNING
The Relation Between Behavior and Payoff
Operant learning has many parallels with Pavlovian learning. As one example, extinction also occurs in operant learning if the reinforcer is omitted following training. Although extinction is once again a useful technique for eliminating unwanted behaviors, just as we saw with Pavlovian learning, it does not destroy the original learning—spontaneous recovery, renewal, reinstatement, and rapid reacquisition effects still obtain. Although early accounts of instrumental learning, beginning with Edward Thorndike, emphasized the role of the reinforcer as “stamping in” the instrumental action, more-modern approaches tend to view the reinforcer as a sort of guide or motivator of behavior. A modern, “synthetic” view of operant conditioning (see later discussion) holds that the organism associates the action with the outcome in much the way that stimulus–outcome learning is believed to be involved in Pavlovian learning.
Human behavior is influenced by a wide variety of reinforcers, including social ones. For example, simple attention from teachers or hospital staff members has been shown to reinforce disruptive or problematic behavior in students or patients. In either case, when the attention is withdrawn and redirected toward other activities, the problematic behaviors can decrease (i.e., undergo extinction). Human behavior is also influenced by verbal reinforcers, like praise, and, more generally, by conditioned reinforcers, such as money, that have no intrinsic value except for the value derived through association with more basic, “primary” rewards. Conditioned reinforcers have been used in schools and institutional settings in so-called token economies in which positive behaviors are reinforced with tokens that can be used to purchase valued items. In more natural settings, reinforcers are always delivered in social relationships, in which their effects are dynamic and reciprocal. For example, the relationship between a parent and a child is full of interacting and reciprocating operant contingencies in which the delivery (and withholding) of reinforcers and punishers shapes the behavior of each. Like Pavlovian learning, operant learning is always operating and always influencing behavior.
Research on operant conditioning in the laboratory has offered many insights into how action relates to its payoff. In the natural world, few actions are reinforced every time they are performed; instead, most actions are reinforced only intermittently. In a ratio reinforcement schedule, the reinforcer is directly related to the amount of work or responding that the organism emits. That is, there is some work requirement that determines when the next reinforcer will be presented. In a “fixed ratio schedule,” every xth action is reinforced; in a “variable ratio schedule,” there is an average ratio requirement, but the number of responses required for each successive reinforcer varies. Ratio schedules, especially variable ratio schedules, can generate high rates of behavior, as seen in the behavior directed at a casino slot machine. In an interval reinforcement schedule,
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


