Of all the disorders characterized by symptoms in the absence of disease, conversion disorders are perhaps the most difficult to explain. How, for example, can one explain functional blindness or a loss of function of both legs in the absence of conspicuous organic disease? The ancient Greeks recognized that if we suffer emotional disturbance as a result of some serious stress (such as personal injury or bereavement), this causes a change in the nervous system which leads in turn to symptoms in different parts of the body according to the underlying pathophysiology. Nineteenth century neurologists made significant advances when they identified specific ideas at the root of the symptoms. In the early nineteenth century Collie(1) also observed that the significance of, and attention to, a symptom or set of symptoms may depend more on what they mean (or their value) to the individual than on the biological underpinnings of the symptom itself.
Spence has recently argued that the problem in hysterical motor disorders is not the voluntary motor system per se: rather, it is in the way that the motor system is utilized in the performance (or nonperformance) of certain willed, chosen, actions.(2) This model invokes a consciousness that acts upon the body and the world. By contrast, the psychodynamic (‘conversion’) model, which Freud introduced and which held sway for most of the twentieth century, invokes an unconscious mechanism ‘acting’ independently of consciousness, to interfere with voluntary movement. Spence has further argued that hysterical paralyses are maintained not by unconscious mechanisms, but by conscious processes. The maintenance of these symptoms requires the patient’s attention, a characteristic of higher motor acts; the paralyses break down when the subject is distracted, consciousness is obtunded, or when it (the ‘paralyses’) is circumvented by reflexive motor routines. Hysterical paralyses, Spence avers, are quintessentially disorders of action (or inactions), which the patient disavows, when faced with some overwhelming situation, which threatens the identity of the self.(2)
One regrettable development of psychiatry’s adoption of Freudian theory was the fracture in communication between the disciplines of psychiatry and neurology, which has only recently been restored by the sort of collaborative research currently being carried out by neurologists and psychiatrists.(3) In the last decade there have also been exciting advances in neuroimaging, which have stimulated research into the neurophysiology of hysteria, and these will be described later. This chapter will also emphasize contemporary approaches to management of these difficult clinical problems.
Problems with definition
There are a number of problems with the definition of the conversion disorders (CD). First, physical disorder must be excluded, but neurological co-morbidity is known to be high in patients with CD,(4) and distinguishing which symptoms are accounted for by organic disease and which are not can be difficult. Second, it is stated that a temporal association between a psychological stressor and the onset on the disorder should be identified, but in practice this is often impossible to establish and depends to a large extent on the skill of the interviewing doctor. Finally, by definition (according to the glossaries ICD-10 and DSM-IV)(5,6); the process should be unconsciously mediated, but it is difficult (some would say impossible) to distinguish between symptoms that are not consciously produced and those that are intentionally manufactured. The DSM-IV provides no criteria to distinguish conscious from unconscious intent, and many authors have argued that the criteria for whether the patients are consciously aware of producing these symptoms should be dropped from the diagnosis of CD.(7)
In clinical practice it is often difficult for a physician, faced with a patient in a hospital bed unable to use his or her legs despite normal tests and clinical findings, to differentiate between conversion disorder, factitious or fabricated disorder, or frank malingering. What the clinician is being asked to do is to determine whether or not the symptoms are being produced intentionally or not; and what the motives are. Table 5.2.4.1 attempts to provide a framework, but it highlights the shortcomings of psychiatric glossaries, which in turn expose the limitations of the medical model, which forces doctors to place patients in categories without taking into account the normal moral capacity of many individuals to exercise choice and determine (at least to some extent) their actions.(8) These medical conundrums have been explored in more detail in the chapter on factitious disorders and malingering (Chapter 5.2.9).
The role of volition
Central to recent debates about hysteria and conversion disorders is the extent to which a person’s illness presentation is considered a product of free will and hence social deviance or the result of psychopathology and/or psychosocial influences beyond the volitional control of the subject.(9) The proposal that voluntary processes are involved in some way has a very long history: something prevents a specific voluntary behaviour from being executed through a ‘negative’, lack of movement (as in paralysis), or a ‘positive’, abnormality of movement (as in psychogenic tremor). If ‘will’ is regarded as a conscious capacity that humans possess to choose what to do or refrain from doing, then the problem in CD appears to be that the will fails to produce normal action.(10) Hence, the diagnostic importance is placed on the patient’s veracity: if we believe him when he says that he cannot act normally we conclude that his will is impeded pathologically; if we do not believe him we conclude instead that his will is deployed to deceive us. This is the distinction required by the diagnostic systems.
Table 5.2.4.1 Relationships between conversion hysteria, factious disorder, and malingering
Subject insight
Target of deception
Perceived outcome
Motivation/reason
Aware
Unaware
Conscious self
Other
Hysterical conversion
+
+
Sick and disabled role
Care/dependency
Factious disorder
+
+
Sick and disabled role
Care/dependency
Malingering
+
+
Sick and disabled role
Personal benefit, e.g. financial, avoiding prison
(Reproduced from Halligan, P. Bass, C. and Oakley, D. Wilful deception as illness behaviour. In Malingering and illness deception (eds. P. Halligan, C. Bass, and D. Oakley), pp. 3-28. Copyright 2003, with permission from Oxford University Press).
Conversion and dissociation
The word conversionis conventionally applied to somatic symptoms whereas if the symptom is psychological (e.g. a loss of memory or an external hallucination) rather than bodily (e.g. a loss of power) it is regarded as dissociative. Dissociation has attracted considerable recent interest, and it has been argued that the available evidence is more consistent with a model that identifies at least two distinct categories of dissociative phenomena—‘detachment’ and ‘compartmentalization’ —that have different definitions, mechanisms, and treatment implications.(11) These have been referred to as Type 1 (compartmentalization) and Type 2 (detachment), respectively (see Table 5.2.4.2).
Compartmentalization phenomena are characterized by impairment in the ability to control processes or actions that would usually be amenable to such control and which are otherwise functioning normally. This category encompasses unexplained neurological symptoms (including dissociative amnesia) and benign phenomena such as those produced by hypnotic suggestion. By contrast, detachment phenomena are characterized by an altered state of consciousness associated with a sense of separation from the self, the body, or the world. Depersonalization, derealization and out-of-body experiences constitute archetypal examples of detachment in this account. Evidence suggests that these phenomena are generated by a common pathophysiological mechanism involving the top-down inhibition of limbic emotional processing by frontal brain systems. Although these two types of dissociation are typically conflated, evidence suggests that different pathological mechanisms may be operating in each case.
Table 5.2.4.2 Classification of two types of pathological dissociation
Type 1 dissociation (compartmentalisation)
Type 2 dissociation (detachment)
Conversion disorders
Depersonalization/derealization
Dissociative amnesia
Peri-traumatic dissociation
Dissociative fugue
Out of body experiences
Dissociative identity disorder
Autoscopy (?)
(Reproduced with permission, from R. Brown (2002))
Support for the compartmentalization model comes from psychophysiological research, which suggests that psychogenic illness is associated with a deficit in attentional, conscious processing and the preservation of preattentive, preconscious processes. According to Brown(12) there is very little difference between ‘negative’ symptoms such as sensory loss, paralysis, etc. and ‘positive’ symptoms such as tremor, dystonia, etc. in terms of basic underlying mechanisms. By this view, all symptoms result from a loss of normal high-level attentional control over low-level processing systems; in this sense, all symptoms can be thought of as involving a form of compartmentalization.
Pathophysiology
There has been considerable progress in cognitive neuroscience and functional imaging over the last decade, which has provided a conceptual and empirically based platform for developing a neuroscience of not only hysterical symptoms but also free will.(13,14)
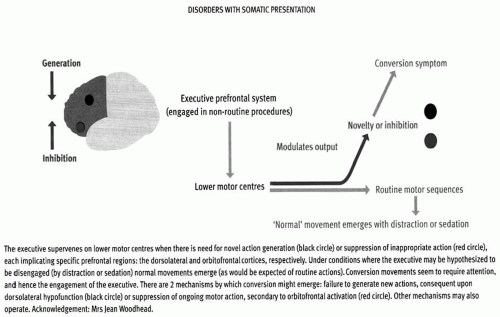
Fig. 5.2.4.1 Schematic diagram illustrating the role of prefrontal executive in modulating lower motor systems, and its hypothesized involvement in conversion disorder. (Reproduced with permission from Spence, S. (2006). Hysteria: a new look. In Psychiatry, 5(2), pp. 56-60, Elsevier Ltd.)
Recent functional neuroimaging data suggest that neural circuits linking volition, movement, and perception are disrupted in CD.(13) There are many studies examining the role of specific prefrontal regions in action generation (particularly the dorsolateral prefrontal and supplementary motor areas) and action suppression (especially the orbitofrontal cortices). These ‘higher’ executive centres supervene only when a change of behaviour is required: inappropriate behaviour must be suppressed or difficult procedures attended to, as when concentration is necessary. Hence, if the problem in hysteria is one of the will, and of abnormality emerging only when subjects attend to their actions, then this suggests the hypothesis that the prefrontal cortex is pivotal to the conversion process (see Fig. 5.2.4.1).
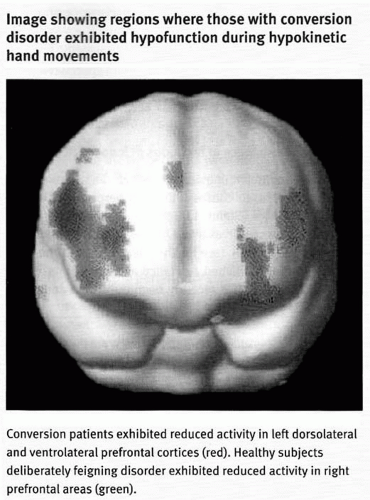
Further evidence that the prefrontal cortices play a key role in the control of action comes from a study of a woman with a left-sided conversion disorder affecting her leg. Marshall et al.(15) demonstrated that her attempt to move her paralysed leg was associated with increased activation of orbitofrontal (inhibitory) prefrontal regions, in the absence of motor cortical activity. They argued for an inhibition of motor behaviour by higher centres. Spence and colleagues(16) demonstrated that in three men with conversion symptoms affecting their upper limbs, hypokinetic movement was associated with reduced activation of dorsolateral (action-generation) areas of prefrontal cortex. Moreover, these areas of hypoactivity differed from those exhibited by four healthy men who were asked to feign the same motor impairments (see Fig. 5.2.4.2). It is possible that the application of functional neuroimaging techniques might allow clinicians to distinguish conversion from feigning on objective, empirical grounds.
Fig. 5.2.4.2 Image showing regions where those with conversion disorder exhibited hypofunction during hypokinetic hand movements. (Reproduced with permission (sought) from Spence, S. (2006). Hysteria: a new look. In Psychiatry, 5(2), pp. 56-60, Elsevier Ltd.
In another recent case report using fMRI a patient with rightsided paralysis was asked to recall traumatic memories using a standard life event schedule: cued recall of the event was associated with regional brain activities characteristic of emotional arousal, including the amygdala and right inferior frontal lobe. Such recall was also associated with reduced motor activity in the area corresponding to the subjective paralysed limb.(17) This case study provides neuroimaging evidence for a connection between traumatic events and ongoing neurological symptoms (see Problems with definition, above).
Epidemiology
It is ironic that these research advances have occurred at a time when social historians have confidently asserted that hysteria has disappeared from clinical practice:
The most consequential development in the history of hysteria in the last century was the rapid decline in the medically recorded incidence of the disorder … … . .Hysteria—considered variously as a term, a theory, and a behaviour—is vanishing.(18)
It is extraordinary that this was written in 2001, at a time when symptoms considered ‘functional, psychogenic, medically unexplained or hysterical’ account for up to a third of new referrals to neurology outpatient departments.(3) and up to 9 per cent of admissions to a UK neurology in patient ward.(19) Akagi and House(20) concluded that the lowest prevalence figures suggested a rate of about 50 per 100 000 for cases of CD known to health services at any one time, with perhaps twice that number affected over a 1-year period. These figures suggest that hysteria is as common as other disabling conditions such as multiple sclerosis and schizophrenia. Furthermore, the burden of disability associated with chronic hysteria is far higher than a typical practising psychiatrist might expect, or than is reflected in standard textbooks of psychiatry or clinical neurology.(21)
It is regrettable therefore that it receives none of the resources or media attention that these disorders attract.
Clinical features
Conversion disorder: motor symptoms
The most typical motor symptoms are paralyses, functional weakness, gait disturbances, fits resembling epilepsy, and abnormal movements.
In the last decade diagnostic procedures have improved and the availability of non-invasive, accurate imaging has drastically reduced the rates of undetected organic pathology in patients with diagnoses of hysteria. Indeed, several recent studies have reported rates of misdiagnosis of between 0 and 4 per cent in regional and tertiary neurological centres,(22) which suggests that a diagnosis of CD can be made relatively confidently and accurately. In the following section the process of diagnosis will be briefly outlined through the history, examination, and investigation.
(a) The history
The onset, temporal sequence, and character of the presenting complaint may not be typical of a neurological disorder, and a number of other features may emerge, especially after an interview with a family member or a review of the hospital and general practitioner notes. If the patient is admitted to a general hospital bed the psychiatrist should routinely telephone the patient’s primary care doctor and request a recent print out of his/her medical records (with consent). These often reveal key information about life events and/or antecedent illnesses, investigations, etc.
(i) Age of onset and sex
The average age of onset is the mid-30s, and patients with functional paralysis are less likely to be female than patients with pseudo seizures.
(ii) Mode of onset/recent life events or difficulties
An increased number of life events in the year preceding symptom onset have been recorded in small controlled studies of unexplained motor symptoms(23,24). When patients are interviewed carefully, some report symptoms of panic just before the onset of, for example, functional weakness.(25) Judicious questions about sensations of sweating, dizziness, and difficulty breathing may reveal these somatic symptoms of anxiety, which may also be reported before the onset of sensory symptoms (see below). There is also an important literature describing unilateral somatic symptoms (which may present with sudden onset of functional weakness in a limb) following hyperventilation/panic.(26,27) These patients may present acutely in the A and E department of a general hospital, where they may be admitted to the hospital stroke unit, or be sent to the general hospital as an emergency with an accompanying letter from the patient’s GP describing the patient as ‘off legs-please see and investigate.’ The following clinical vignette is typical:
A 40-year-old woman was admitted as an emergency to the Stroke unit of the general hospital after collapsing at home. She had been involved in a dispute with her employers for weeks, and on the morning of the referral had an argument with her mother which made her very upset, and during the course of this she became distressed and developed paraesthesiae down the left side of her body, slurred speech, and collapsed, losing consciousness for 30 s. An ambulance was called and she was admitted to the A and E department, where she was noted to be hyperventilating and agitated, and to have weakness of the left leg, unintelligible speech, and claimed not to be able to see. All neurological investigations were normal, and after 12 days in hospital she made a gradual recovery, but was left with functional weakness in the left leg (requiring a wheelchair), and her speech was intermittently ‘child-like’. History revealed a similar episode 3 years previously, a recent 2-year history of treatment for irritable bowel syndrome, and considerable work and domestic stress.
She was followed up by the liaison service and community mental health team, but despite the efforts of a community physiotherapist, psychologist, and nursing support her limb weakness continued and she remained disabled; 1 year after admission she was in receipt of disability benefits.
(iii) Previous unexplained symptoms
Evidence is accumulating that the more unexplained symptoms the patient has, the more likely the primary symptom is to be unexplained by disease.(28) In a recent study of patients with medically unexplained motor symptoms, additional unexplained symptoms including paraesthesia (65 per cent), pseudo epileptic seizures (23 per cent), and memory impairment (20 per cent) were reported.(4) It is often useful therefore, when CD is being considered as a diagnosis, to obtain a print out of the patient’s past history from the primary care doctor (having obtained the patient’s consent). This may reveal repeated presentations to different specialists as well as a history of repeated surgical procedures, particularly without clear evidence of pathology. It is also worth noting that patients with a diagnosis of somatization disorder (what used to be referred to as Briquet’s syndrome) have high rates of conversion disorders, which punctuate their illness careers, often after a life event or physical injury/procedure.(29)
Only gold members can continue reading. Log In or Register to continue